What is an allergy to a vaccine?
Traditionally, allergic reactions to vaccines can be divided into local and general.
- Locally, redness at the injection site and the formation of a small compaction are possible. If the diameter of the red spot does not exceed 2.5 cm, then the allergic reaction is considered mild and does not require contact with an allergist. If the diameter of the spot is more than 2.5 cm, but less than 5, then this reaction is considered average. When a red lump more than 5 cm in diameter forms, the allergic reaction is considered severe and requires immediate consultation with a specialist.
- Among the common reactions that occur after vaccination against hepatitis B, it is worth noting a slight rise in temperature, fatigue, headache and aches in muscles and joints, dizziness and nausea. The severity of these reactions is traditionally determined depending on the temperature indicator. Up to 37.50C – weak reaction, up to 38.50C – medium and further – high.
It is worth noting that the previously described cases of autism or multiple sclerosis after the administration of a hepatitis vaccine do not refer to allergic reactions. In addition, these cases were never properly confirmed in medical practice, since they were not accompanied by the appropriate evidence base.
Problems of vaccination of children with allergic diseases
The only way to reduce the incidence of vaccine-preventable infections and prevent the development of epidemics at the present stage is 95% coverage of the population with preventive vaccinations. This means that not only healthy children, but also children suffering from various diseases are subject to vaccination.
The current opinion that vaccines are “allergenic” is valid only in relation to some of the substances they contain. Progress in the production of vaccines frees them to a greater extent from ballast substances: due to better purification, all vaccines included in the National Vaccination Calendar contain much less antigens than vaccines in the 20s and 30s. Both live and inactivated vaccines practically do not stimulate a persistent increase in IgE levels and the production of specific IgE antibodies.
The wide prevalence of allergic pathology in children, the annual increase in the number of patients in the pediatric population, the early onset, often in the first year of life, and the chronic nature of the disease have led to the fact that pediatricians constantly need to vaccinate children with allergic diseases. Currently, the attitude towards vaccination of children with allergy pathology has radically changed for the better. However, the lack of personal experience of practicing doctors, both in the tactics of treating such children and in approaches to carrying out preventive vaccinations for various forms and severity of the disease, puts the doctor in a difficult position when it comes to choosing vaccination tactics for these patients.
When deciding on the timing of vaccination, the volume of drug preparation and the choice of vaccine preparation, it is necessary to take into account the spectrum of sensitization, nosological form and stage of the disease, that is, the basis of the tactics of vaccinating children with allergic diseases is an individual approach to each child. However, despite the polymorphism of atopy manifestations, the immunization of these children is guided by a number of general principles:
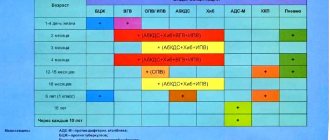
- Children with allergic diseases are subject to vaccination against all infections included in the preventive vaccination calendar (tuberculosis, viral hepatitis B, diphtheria, tetanus, whooping cough, polio, measles, mumps, rubella) in accordance with available instructions. Both domestic and foreign vaccine preparations are used for immunization. In this case, preference is given to combined vaccines (for example, measles-mumps divaccine or trivaccines (“Priorix”, “M-M-PII”) against measles, mumps and rubella), which allows to reduce the total volume of administered preservatives.
- In most cases, for children with allergic diseases, especially those with damage to the respiratory tract, it is advisable to expand the schedule of preventive vaccinations through annual vaccination against influenza, as well as against pneumococcal and Haemophilus influenzae infections. Vaccination against these infections leads not only to a reduction in the frequency and severity of intercurrent diseases, but also contributes to the positive dynamics of the course of the underlying disease, allowing for a reduction in the volume of basic therapy and an extension of the period of remission. The introduction of additional vaccine preparations can be combined with vaccines from the main vaccination schedule.
- A history of systemic allergic reactions to antibiotics contained in vaccines and to culture substrate antigens (in particular, chicken and/or quail egg white) in children with allergic diseases is a contraindication for the administration of measles and mumps vaccines. Identification of a severe allergy to chicken egg proteins in patients is also a contraindication for vaccination with influenza vaccines against tick-borne encephalitis prepared on a chicken substrate.
It is important to remember that the presence of a documented allergy to the listed components is not a clear contraindication to immunization with vaccines containing them; the nature of these reactions is also important. For example, if when trying to eat an egg, swelling of the lip or an anaphylactic reaction immediately occurs, then vaccination is absolutely contraindicated. If the allergy manifests itself as reactions of minor severity, then in most cases such patients can be vaccinated against the background of prophylactic administration of antiallergic drugs.
Severe allergic reactions to baker's yeast may be a contraindication for vaccination against viral hepatitis B, because yeast is used in the production of the main antigen and can be found in purely symbolic quantities in vaccines.
- Vaccination of children with allergic diseases is carried out when complete or partial remission is achieved; in the latter case, we are talking about the patient maintaining mild clinical manifestations without signs of exacerbation of the disease.
Children suffering from hay fever are given preventive vaccinations outside the dusting season of causally significant plants.
Vaccination of children with allergic diseases that are not seasonal is carried out at any time of the year, however, taking into account the epidemic situation, it is advisable to vaccinate children who often suffer from respiratory infections in warm years, outside the period of high incidence of acute respiratory viral infections (ARVI). The development of ARVI in one of the family members in a favorable epidemiological situation serves as the basis for a temporary (until their recovery) exemption from preventive vaccinations for children with allergic diseases.
According to epidemic indications, children with allergy pathology can be vaccinated during the period of exacerbation of the disease. In such cases, vaccination is carried out under the supervision of an allergist-immunologist.
- Preventive vaccinations for children with this pathology should be carried out against the background of basic therapy, the volume and duration of which depend on the period and severity of the allergic disease. It should be emphasized that long-term use of topical glucocorticosteroid drugs (inhaled, endonasal, conjunctival or cutaneous) is not a contraindication to the administration of vaccine drugs.
In all cases, one of the antimediator drugs is prescribed in an age-specific dosage for 3–5 days before and after vaccination, preference is given to 2nd and 3rd generation drugs. In the case of live vaccines (due to the later onset of adverse reactions), the use of antihistamines can continue for 2-3 weeks after vaccination.
- A high risk factor for the occurrence of severe manifestations of allergy to vaccine preparations is the development of systemic allergic reactions in the post-vaccination period in the form of generalized urticaria, Quincke's edema, and anaphylactic shock. Children who experience anaphylactic shock upon administration of the vaccine are subject to exclusion from subsequent immunization with this drug. The issue of continuing immunization of children who have systemic manifestations of allergies in the form of urticaria and allergic edema in the post-vaccination period is decided in each specific case individually, after consultation with an allergist. According to epidemiological indications, such children can be revaccinated during the period of remission of an allergic disease against the background of preventive antiallergic therapy, including parenteral administration of antihistamines, glucocorticosteroids, and adrenaline immediately before the vaccine is administered.
- Preventive vaccinations for children with allergic diseases should be carried out in immunization rooms, vaccination rooms, first aid stations (FAP) or in hospitals if anti-shock therapy is available. After each vaccination, the child should be under the supervision of medical personnel for at least 30 minutes, since during this period immediate systemic allergic reactions, which are the most dangerous for the patient, may develop.
- During the vaccination period, children are recommended to follow a diet excluding obligate allergens and histamine liberators (fish, eggs, honey, chocolate, nuts, cocoa, citrus fruits, strawberries, wild strawberries), and also refrain from taking other products to which allergic reactions have previously been noted, not including while introducing new foods into the diet. The diet is followed for at least 1 week before vaccination and 1–3 months after it (depending on the type of vaccine preparation and the course of the post-vaccination period).
- Skin tests with non-infectious and infectious allergens can be performed 1.5 weeks before the administration of vaccine preparations or 1-1.5 months after it.
- If a child receives a course of allergen-specific immunotherapy, as well as a course of therapy with Histaglobulin, Allergoglobulin or Antiallergic immunoglobulin, then vaccination should be carried out no earlier than 1–1.5 months after completion of the course of treatment, except in situations due to epidemiological indications. After the introduction of vaccine preparations, courses of therapy can be started no earlier than 1 month (with the introduction of live viral vaccines - after 1.5–2 months).
- After performing the Mantoux test, the administration of vaccine preparations (with the exception of BCG and BCG-M) is recommended no earlier than 10–12 days, since most children with allergic pathology have a positive reaction to tuberculin, indicating the presence of an allergic altered reactivity in the child, with For immunization due to epidemiological indications, this period may be shorter. After administration of the DTP vaccine, ADS, ADS-M toxoids, LCV (live measles vaccine) and mumps vaccine, the Mantoux test can be performed no earlier than 1.5 months later, i.e. period of recovery of immunological status indicators in children with allergic diseases.
- For children with an irregular vaccination schedule who have had a history of one vaccination with DPT vaccine or DPT, ADS-M toxoids, regardless of the time elapsed after it, it is enough to administer another dose of DTP or ADS-M toxoids, followed by revaccination after 6 months. The choice of vaccine depends on the age of the child. If children have a history of two vaccinations with DPT vaccine or ADS, ADS-M toxoid, revaccination with ADS or ADS-M toxoid should also be carried out without taking into account the time that has passed since the last vaccination, but not earlier than 6–12 months.
- The experience of vaccinating children with allergic diseases, which we have accumulated over many years of practice (from 1984 to the present) in the laboratory of vaccine prevention and immunotherapy of allergic diseases, State Research Institute of Vaccines and Serums named after. I.I. Mechnikov RAMS, indicates that immunization carried out during the period of complete remission of the disease in accordance with the above recommendations is practically not accompanied by post-vaccination complications or exacerbation of allergopathology.
A moderate exacerbation of the underlying disease was recorded only in patients with atopic dermatitis, in whom vaccination was carried out during unstable remission or during a subacute course. The frequency of exacerbation of atopic dermatitis was 8.6% after administration of the DPT vaccine, 10–21% after immunization with ADS-M toxoid, 4.5% after vaccination against measles and mumps. The immunization did not worsen the course of the allergic disease. Our experience has shown that such manifestations were short-lived and did not affect the course of the post-vaccination period during subsequent immunization.
Clinical observation of patients with bronchial asthma in the post-vaccination period showed that asthma attacks did not occur in any of the observed groups. A study of bronchial patency in 195 patients over 5 years of age during the full course of immunization with ADS-M toxoid confirmed that vaccination does not lead to an exacerbation of the underlying disease, even in the presence of obvious or hidden signs of bronchospasm. General mild and moderate reactions were recorded in 30 (14.5%) patients, mild allergic rashes in 10 (2.9%) patients, local infiltrates measuring 5x5 cm in 15 (4.4%) children, a combination general and local reactions - in 10 (2.9%) cases. The probability of their occurrence did not depend on the duration of the remission period and corresponded to that during vaccination of healthy children with ADS-M toxoid. Therapy prescribed in the post-vaccination period, taking into account spirography data and the clinical picture, not only prevented the development of repeated attacks of asthma, but also, in some cases, contributed to the temporary normalization of bronchial patency. Thus, in patients who had signs of bronchial obstruction before vaccination, in the post-vaccination period the indicators of bronchial patency normalized and remained so for more than 6 months.
We vaccinated children against diphtheria and tetanus with a history of allergic urticaria and angioedema. Clinical observation carried out in the post-vaccination period for 6–12 months did not reveal a single case of recurrence of angioedema and urticaria, despite the fact that the duration of the period of remission of the disease at the time of vaccination varied from 1 week to 3 or more months.
When analyzing the reactions that occurred in children with allergic diseases within one month after the administration of the measles vaccine according to an individual regimen, it was possible to identify only a mild allergic rash in the first week after vaccination in 10.6% of those vaccinated for 4–5 days, and only in one The patient noted a moderate exacerbation of dermatitis within one week. Among children with bronchial asthma and hay fever, vaccination was not accompanied by exacerbation of the disease or the occurrence of any allergic reactions. Currently, there is evidence from additional studies confirming that vaccination against measles in children with bronchial asthma of any severity is safe and effective if carried out against the background of treatment of the underlying disease.
It is known that patients with allergies are more susceptible to tuberculosis, and among patients with tuberculosis, allergic pathology occurs 4 times more often than in people who are not sick. The combination of tuberculosis with bronchial asthma causes a particularly severe course of the latter. Thus, it is possible that anti-tuberculosis vaccination and revaccination are especially indicated for patients with asthma. For revaccination against tuberculosis in children suffering from allergic pathology, the BCG-M vaccine is used. Revaccination carried out during a period of stable remission of the allergic process is not accompanied by an exacerbation of the underlying disease. The BCG-M vaccine, in addition to its specific protective effect, has a pronounced immunomodeling effect, which, in turn, helps reduce the incidence of intercurrent acute respiratory viral infections and associated exacerbations of bronchial asthma.
A full course of vaccination against hepatitis B was administered to 40% of children with atopic dermatitis, 30% with bronchial asthma, 20% with seasonal and year-round allergic rhinoconjunctivitis, 10% with urticaria and Quincke's edema with varying severity of the underlying disease against the background of basic therapy . In the post-vaccination period, no unusual reactions or complications, including exacerbation of the underlying disease, were observed.
Children with allergic diseases, especially those suffering from bronchial asthma, need protection from acute respiratory infections, incl. flu According to WHO recommendations, all patients with bronchial asthma should be vaccinated against influenza annually, regardless of the form and severity of the disease or drug therapy. We did not detect repeated asthma attacks in the post-vaccination period or the occurrence of other reactions during influenza vaccination. Studies have not demonstrated deterioration in respiratory function, increased asthma symptoms, or increased use of drug therapy. Local reactions (in the form of pain at the site of vaccine administration) and a general mild reaction (fever up to 37–37.2°C) were detected in 10% of cases, and no drug treatment was required. In 2% of cases, an allergic rash developed, which quickly disappeared with the use of Claritin. When observing children for 6 months after vaccination, ARVI was noted in 5% of cases (serological identification was not carried out). For comparison, during the same period of time before vaccination, children suffered from ARVI 3-6 times a year.
The most effective in children with bronchial asthma was the combined use of vaccines against influenza and pneumococcal infection. When vaccinating children with varying severity of bronchial asthma with Vaxigrip and Pneumo 23, there was a decrease in the frequency of exacerbations of the disease by 1.7 times, the number of intercurrent respiratory infections by 2.5 times, and an improvement in external respiratory function indicators (FEV1, SOS25–75 and SOS75–85). At the same time, in the dynamics of the vaccination process, no changes in the content of eosinophils in the peripheral blood and the results of skin prick tests were detected.
Vaccination against meningococcal infection of serogroups A+C is recommended by us to all children after completing the full course of vaccination, according to the national vaccination schedule. As a rule, this coincides with the child’s entry into kindergarten and, less often, school. We observed more than 120 children of various ages (over two years old) with various allergic diseases. Vaccination was carried out with the drug “Polysaccharide meningococcal vaccine A+C” during the period of remission of the disease and, as always, against the background of a short course of antimediator drugs. In the clinical aspect, the introduction of the Polysaccharide meningococcal vaccine A+C, like any other polysaccharide vaccine, was accompanied by the occurrence of mild local reactions (no more than 3–4% of cases) and almost the same frequency of general mild temperature reactions. Allergic diseases did not worsen due to vaccination.
It is characteristic that the concentration of total IgE in the post-vaccination period increased briefly and after 1.5–2 months returned to the original values. A transient increase in the level of total IgE was observed mainly in children who had general or local allergic reactions in the post-vaccination period.
The administration of vaccine preparations to children with allergic diseases is accompanied by the synthesis of antibodies to vaccine antigens at the level of protective values, as in healthy children.
Thus, the studies not only confirm the possibility, but also indicate the need for active immunization of children with allergy pathology. Allergic diseases are an indication for vaccination rather than a contraindication, since in these children the infections are especially severe (for example, whooping cough in a patient with asthma). A pediatrician, when consulting such a child with an allergist, should raise the question not about the admissibility of vaccinations, but about choosing the optimal time for their implementation and the need for medicinal protection (antihistamines for cutaneous forms of atopy, inhaled steroids and beta-agonists for asthma).
It should be emphasized that neither the presence of allergopathology nor the development of post-vaccination reactions or exacerbation of an allergic disease after the administration of vaccine preparations is an absolute contraindication to future preventive vaccinations.
Literature
- Medunitsin N.V. Vaccinology. M.: Triad-H. 1999. 272 p.
- Fundamentals of vaccine prevention in children with chronic pathology / Ed. M. P. Kostinova. M.: Medicine for everyone. 2002. 320 p.
- Martishevskaya E. A. Clinical and immunological characteristics of the measles vaccination process in children with bronchial asthma. Author's abstract. Ph.D. honey. Sci. St. Petersburg 2001. 22 p.
- Pukhlik B. M. The relationship between tuberculosis and allergic diseases // Probl. tuberk. 1983. No. 11. pp. 29–32.
- Ala'Eldin H., Ahmed A., Karl G. et al. Influenza vaccination in patients with asthma: effect on peak expiratory flow, asthma symptoms and use of medication. Vaccine 1997; 15:1008–1009.
- Markova T. P., Chuvirov D. G. Use of the Influvac vaccine for the prevention of influenza in children with allergic diseases // Russian Bulletin of Perenatology and Pediatrics. 2001.
- Karpocheva S.V., Andreeva N.P., Magarshak O.O. et al. The course of bronchial asthma and “Vaxigrip” // XIII Russian National Congress “Man and Medicine”: Abstracts. M. 2006. P. 534.
- Guidelines No. 3.3.1.1095-02. Medical contraindications to preventive vaccinations with drugs from the national vaccination calendar.
O. O. Magarshak , Candidate of Medical Sciences M. P. Kostinov , Doctor of Medical Sciences, Professor of the Research Institute of Vaccines and Serums named after. AND.
and Mechnikov RAMS , Moscow
What causes allergies?
The inactivated virus itself practically cannot become a source of antigens. People with an allergy to chicken egg white are at risk for having an allergic reaction to the virus’s envelope proteins. This type of intolerance is not very common.
More often, other components of the vaccine are responsible for hypersensitivity reactions, which are added to ensure its stability and prevent microbial contamination.
- Merthiolates are sulfur compounds added as a preservative.
- Aluminum hydroxide.
- Traces of yeast proteins. People with a history of yeast allergies should be careful in preparation before vaccination. Such intolerance is determined using a special allergen test.
Should a child with allergies be vaccinated?
Of course it's worth it! Children with allergies are much more susceptible to infectious diseases, so they should be vaccinated first. But you need to vaccinate with caution, although atopic dermatitis, food allergies, hay fever are not contraindications to vaccination.
Before vaccination, a child with allergies is examined by a pediatrician, immunologist, dentist, neurologist and ENT specialist. A general blood and urine test is prescribed.
Vaccination is carried out without exacerbation of an allergic disease.
The interval between vaccinations must be at least 30 days. After the Mantoux test, 3 days should pass.
How to prepare a child for vaccination?
Vaccinations can be emergency or scheduled (for example, DTP). Emergency vaccination is indicated for people at high risk of infection and for epidemiological reasons. For example, in case of bites from dogs and wild animals, emergency vaccination against rabies is carried out, and in case of injuries, burns and wounds, emergency vaccination against tetanus is carried out.
During the season of tick activity, people planning a trip to endemic areas are given emergency prevention of tick-borne encephalitis.
In general, in emergency cases there is no question of any preparation; there is simply no time for it. But with routine vaccinations, it is possible and necessary to prepare a child for future vaccinations.
Remember:
- Try to avoid “food experiments” and not introduce new foods into your baby’s diet. For example, citrus fruits, nuts, eggs;
- Do not overload your baby with rich and high-calorie food before and after vaccination;
- A few days before vaccination (and after it), limit your child’s communication with other children and adults, avoid public transport, shops and crowded events, so as not to “catch” the infection;
- Before vaccination, a child with allergic diseases receives “medicinal preparation” consisting of antihistamines (diazolin, tavegil, loratadine, etc.), calcium gluconate and decoctions of medicinal herbs (dandelion, burdock root, valerian, licorice);
- To reduce the risk of developing “vaccine allergy,” pediatricians (Protsyuk T.L. et al., 2011) also recommend starting to take Enterosgel in an age-weight dosage 7 days before vaccination (see instructions for use). The course of the drug is continued on the day of vaccination and a couple of days after it.
- Vaccinated children should be protected from hypothermia and excessive physical stress.