Description of the drug
The Infanrix Hexa vaccine is one of the most modern combination vaccines, which allows you to simultaneously protect a child from six dangerous infections. The vaccine has been successfully used in Europe for about 10 years and meets all WHO requirements for the production of biological substances.
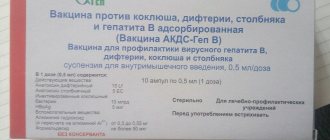
Infanrix Hexa is an adsorbed acellular (acellular) diphtheria-tetanus-pertussis vaccine, inactivated polio vaccine, recombinant hepatitis B vaccine and a vaccine for the prevention of Haemophilus influenzae type b.
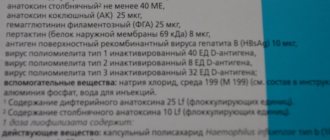
The Infanrix Hexa vaccine contains diphtheria and tetanus toxoid antigens, components of the cell wall of the causative agent of whooping cough, inactivated polio virus types 1,2,3, capsular polysaccharides of Haemophilus influenzae type b, and genetically engineered HbsAg (hepatitis B antigen).
Using the most modern technologies in the production of Infanrix Hexa, it was possible to reduce the number of protein molecules by 30 times (compared to whole-cell vaccines - DPT) without loss of immunogenicity, which has been proven in numerous clinical studies for each component. With the same effectiveness as whole cell vaccines (DTP), the number of adverse reactions after vaccination with Infanrix Hexa is significantly reduced. The presence of six components in one vaccine allows you to minimize the number of injections, thereby significantly reducing the number of complications and discomfort in the child.
Infanrix® Hexa (Infanrix® HEXA)
Immunogenicity
The immunogenicity of the Infanrix® Hexa vaccine was assessed in clinical studies in children aged 6 weeks and older using two-dose and three-dose primary vaccination regimens followed by booster vaccination. Summarized results of clinical studies are presented in tables.
When using a three-dose primary vaccination regimen, the protective level of antibodies to each of the vaccine antigens was determined in at least 95.7% of vaccinated children. After revaccination, the protective level of antibodies to each of the vaccine antigens was determined in at least 98.4% of vaccinated children.
1 month after completion of the three-dose primary course of vaccination followed by revaccination, the protective titers were:
| Antibodies (protective titer) | 3 doses | 4 doses (booster vaccination in the second year of life after a three-dose primary vaccination) | ||
| 2-3-4 months N=196 (2 studies) | 2-4-6 months N = 1693 (6 studies) | 3-4-5 months N=1055 (6 studies) | N = 2009 (12 studies) | |
| % | % | % | % | |
| to diphtheria toxoid (0.1 IU/ml) | 100,0 | 99,8 | 99,7 | 99,9 |
| to tetanus toxoid (0.1 IU/ml) | 100,0 | 100,0 | 100,0 | 99,9 |
| to pertussis toxoid (5 ELISA U/ml) | 100,0 | 100,0 | 99,8 | 99,9 |
| to hemagglutinin filamentous (5 ELISA U/ml) | 100,0 | 100,0 | 100,0 | 99,9 |
| to pertactin (5 ELISA U/ml) | 100,0 | 100,0 | 99,7 | 99,5 |
| to hepatitis B virus surface antigen (HBsAg) (10 mIU/ml) | 99,5 | 98,9 | 98,0 | 98,4 |
| to polio virus type 1 (dilution 1: | 100,0 | 99,9 | 99,7 | 99,9 |
| to poliovirus type 2 (dilution 1: | 97,8 | 99,3 | 98,9 | 99,9 |
| to poliovirus type 3 (dilution 1: | 100.0 | 99,7 | 99,7 | 99,9 |
| to capsular polysaccharide Haemophilus influenzae type b (0.15 µg/ml) | 96,4 | 96,6 | 96,8 | 99,7 |

N is the number of vaccinated people;
* in the subgroup of children who did not receive a vaccine to prevent hepatitis B at birth, the protective titer (≥10 mIU/ml) was determined in 77.7%.
After completion of vaccination using a two-dose primary vaccination regimen followed by revaccination with the Infanrix® Hexa vaccine, the protective level of antibodies to each of the vaccine antigens was determined in at least 97.9% of vaccinated people.
1 month after completion of the two-dose primary course of vaccination followed by revaccination, the protective titers were:
| Antibodies (protective titer) | 2 doses and revaccination (2-4-12 months) N=196 (1 study) | 2 doses and revaccination (3-5-11 months) N=352 (3 studies) |
| % | % | |
| to diphtheria toxoid (0.1 IU/ml) | 100,0 | 100,0 |
| to tetanus toxoid (0.1 IU/ml) | 100,0 | 100,0 |
| to pertussis toxoid (5 ELISA U/ml) | 99,5 | 100,0 |
| to hemagglutinin filamentous (5 ELISA U/ml) | 100,0 | 100,0 |
| to pertactin (5 ELISA U/ml) | 100,0 | 99,2 |
| to hepatitis B virus surface antigen (HBsAg) (10 mIU/ml) | 99,8 | 98,9 |
| to polio virus type 1 (dilution 1: | 98,4 | 99,8 |
| to poliovirus type 2 (dilution 1: | 98,4 | 99,4 |
| to poliovirus type 3 (dilution 1: | 97,9 | 99,2 |
| to capsular polysaccharide of Haemophilus influenzae type b (0.15 µg/ml) | 100,0 | 99,6 |
N is the number of vaccinated people.
Serological correlates of protection have been identified for diphtheria, tetanus, polio, hepatitis B virus and Haemophilus influenzae infection. For pertussis, there is no serological correlate of protection.
Because the immune response to the pertussis antigens in Infanrix® Hexa is equivalent to that of the pertussis antigens in Infanrix®, the protective efficacy of the two vaccines is expected to be similar.
Protective efficacy against pertussis
The protective effectiveness of the Infanrix® vaccine against whooping cough ranges from 84% to 88.7%, which is confirmed by the results of clinical studies conducted in Italy (2-4-6 months) and Germany (3-4-5 months). In Italy, following completion of a primary pertussis vaccination regimen without booster vaccination, protective efficacy was maintained for 60 months in the same group of individuals.
Immunogenicity in premature infants
The immunogenicity of the Infanrix® Hexa vaccine was assessed in clinical studies on
after completion of a three-dose primary vaccination course (2-4-6 months) in approximately 300 premature infants (born 24 to 36 weeks). The immunogenicity of the vaccine after booster vaccination at 18 to 24 months of age was assessed in approximately 200 preterm infants.
1 month after completion of the primary vaccination course, at least 98.7% of vaccinated people achieved a level of seroprotection against diphtheria, tetanus and polio virus types 1 and 2; protective level of antibodies to the viral hepatitis B antigen, to the capsular polysaccharide of Haemophilus influenzae
type b, poliovirus type 3 was identified in at least 90.9% of vaccinated people; all vaccinated people were seropositive for filamentous hemaggluginin and pertactin, 94.9% of vaccinated people were seropositive for antibodies to pertussis toxoid.
1 month after revaccination, at least 98.4% of vaccinated people had a protective level of antibodies to each of the vaccine antigens, except for pertussis toxoid (in at least 96.8%) and hepatitis B virus antigen (in at least 88.7%) . The response to the administration of a booster dose in terms of an increase in antibody concentration (15-235 times) indicates the adequacy of primary vaccination against all antigens included in the Infanrix® Hexa vaccine.
In the study, approximately 2.5-3 years after revaccination, 85.3% of vaccinated people maintained the level of seroprotection against the hepatitis B virus and at least 95.7% against poliovirus types 1, 2, 3 and capsular polysaccharide Haemophilus influenzae
type b.
Duration of immune response
The duration of the immune response after completion of a three-dose course of primary vaccination followed by revaccination with the Infanrix® Hexa vaccine was assessed in children aged 4-8 years. Immune protection against poliovirus types 1, 2, 3 and capsular polysaccharide of Haemophilus influenzae
type b was observed in no less than 91.0% of children, against diphtheria and tetanus - in no less than 64.7% of children. No less than 25.4% (antibodies to pertussis toxoid), 97.5% (antibodies to PHA), 87.0% (antibodies to PRN) of children remained seropositive to the pertussis components of the vaccine.
Immune protection against viral hepatitis B after completion of a three-dose course of primary vaccination followed by revaccination with the Infanrix® Hexa vaccine was observed in more than 85% of vaccinated children aged 4-5 years and in more than 72% of vaccinated children aged 7-8 years. After completing a two-dose course of primary vaccination followed by revaccination, immune protection against viral hepatitis B was observed in more than 48% of vaccinated children aged 11-12 years.
With regard to viral hepatitis B, preservation of immune memory in children aged 4-12 years has been confirmed. These children received a course of primary vaccination followed by revaccination with the Infanrix® Hexa vaccine; after administration of an additional dose of a monovalent vaccine for the prevention of viral hepatitis B, the induction of immune protection was noted in at least 96.8% of those vaccinated.
Post-marketing surveillance data
Efficacy of the Infanrix® Hexa vaccine against infection caused by Haemophilus influenzae
type b was assessed in a post-marketing observational study in Germany and was found to be 89.6% for those receiving primary vaccination and 100% for those receiving primary and booster vaccination.
The Infanrix® Hexa vaccine has been used in Italy since 2006 to prevent whooping cough in children aged 3, 5, 11 months of age, vaccination coverage is over 95%. Satisfactory control of Haemophilus influenzae infection remains: from 2006 to 2011 in Italy, no more than 3 confirmed cases of Haemophilus influenzae infection were detected annually in children under 5 years of age.
Vaccination scheme
The primary vaccination regimen consists of three doses of 0.5 ml (vaccine administration at the age of 2–3–4 months; or 3–4–5 months; or 2–4–6 months) or two doses (vaccine administration at the age of 3 ; 5 months). There should be an interval of at least 1 month between doses. Infanrix Hexa administered according to the EPI (Expanded Program on Immunization; 6–10–14 weeks of age) schedule can only be used if the vaccine recipient has received a dose of hepatitis B vaccine at birth.
After vaccination with two doses (eg at 3–5 months of age) of Infanrix Hexa, a booster dose should be given at least 6 months after the last primary dose, preferably between 11 and 13 months of age. After vaccination with three doses (eg, 2–3–4 months; 3–4–5 months; 2–4–6 months) of Infanrix Hexa, a booster dose should be given at least 6 months after the last primary dose, preferably under the age of 18 months.
Directions for use and doses
A single dose is 0.5 ml, contained in a specially designed syringe. This syringe dose of the Infanrix vaccine is aseptically packaged and adapted for convenient transportation and storage, equipped with a special needle that minimizes pain from the injection. The use of such a syringe eliminates overdose and reuse.
The Infanrix vaccine is administered intramuscularly into the thigh. Injection into the buttock is not currently practiced. Intravenous administration is strictly contraindicated.
Contraindications
Only a doctor can decide whether Infanrix Hexa is suitable for vaccination
Vaccination with Infanrix Hexa is contraindicated if there is a history of an allergic reaction to any component of the vaccine, as well as in the following cases:
- Hypersensitivity to the active substances or to any excipients.
- Hypersensitivity after previous vaccination against diphtheria, tetanus, whooping cough.
- Case of encephalopathy within 7 days after any pertussis vaccination.
Possible side effects
The most commonly observed side effects are:
- decreased or complete loss of appetite
- the injection site may become red and painful, and swelling may occur
- the child may become restless and irritable and cry for a long time
- increase in body temperature to 39.5 degrees
More rare manifestations of a reaction to the vaccine:
- vomiting and diarrhea
- the appearance of thickening and redness at the vaccine site
- allergic reaction
Come get vaccinated at MAMARADA. A full range of vaccines for children and adults, family vaccinations - at a special price!
Our doctors
Pastushnaya Victoria Sergeevna
Pediatrician, Chief Physician, Expert, Vaccine Prevention
Gammel Elizaveta Nikolaevna
Pediatrician, Vaccine prevention, Gastroenterologist, Functional diagnostics (Taganka, Zhulebino)
Ilyina Larisa Anatolyevna
Pediatrician, Vaccine prevention (Zhulebino)
Konovalova Elena Borisovna
Pediatrician, Vaccine prevention (Zhulebino)
Filippov Andrey Nikolaevich
Pediatrician, Vaccine prevention (Taganka)
Leave a request
we will find a convenient time for you