Diagnostics
An infectious disease specialist or pediatrician diagnoses the current pathology based on:
- analysis of patient complaints;
- medical history;
- general examination: hyperemia is detected in the throat, palatine arches, signs of inflammation in the epiglottis, subcutaneous fat;
- bacteriological culture of pus, sputum, cerebrospinal fluid, materials taken from mucous membranes on special nutrient media;
- serological diagnostics - antibodies to the pathogen are determined in the blood;
- detection of influenza DNA in sputum and blood plasma using the polymerase chain reaction method;
- consultation with an otolaryngologist.
Haemophilus influenzae infection in children
Depending on where the process is localized, hemophilus influenzae infection provokes meningitis, pneumonia, osteomyelitis, otitis media, acute epiglottitis. Frequent clinical forms for newborns are conjunctivitis, septicemia, purulent arthritis, mastoiditis, etc.
Pneumonia caused by N. influenzae is recorded in 5% of all cases of pneumonia. The disease mainly affects children under 2 years of age. The disease has an acute onset, body temperature is greatly elevated, catarrhal symptoms and severe toxicosis are observed. The symptoms are similar to those of other pneumonia of a bacterial nature.
Percussion and auscultation can detect a focus of inflammation in the projection of one or several segments of the lungs. Most often, the process is localized in the hilar zones, but can affect the lower and upper lobes of one or both lungs. There is a possibility of abscess formation. The radiograph shows foci of homogeneous darkening or dense focal-confluent shadows in the event of exudative pleurisy.
Changes in the blood may vary and depend on each individual case. In some cases, a high leukocyte count, a neutrophil shift and an ESR above normal are found. But in more frequent cases, the number of leukocytes is normal or slightly increased, and the ESR only tends to increase.
Positive blood cultures and pleural effusions are considered critical in diagnosis.
Meningitis caused by N. influenzae is the main causative agent of purulent meningitis in children under 3 years of age. The main risk group is babies in the first months of life. The symptoms of this meningitis are similar to those of other purulent meningitis. The disease begins acutely, with fever (temperature reaches 39-40 °C), the appearance of general infectious toxicosis with repeated vomiting, complete sleep disturbance, agitation, tremor of the hands and chin.
Babies up to 4 months may have bulging of the large fontanelle, hyperesthesia, and in more rare cases, stiff neck muscles and positive Kernig and Brudzinsky symptoms are noted. Changes in the cerebrospinal fluid are very little different from changes in meningococcal or pneumococcal meningitis.
Hemophilic meningitis in children, as a rule, is severe. Fatalities are common. In survivors, the following residual effects are recorded: convulsive syndrome, paralysis, decreased intelligence, increased excitability, hearing impairment, speech impairment, etc.
Panniculitis is also known as cellulite . This is an inflammation of fatty tissue in children under 12 months. The onset of the disease is characterized by the appearance of dense painful areas of bluish-red or purple color with a diameter of 1 to 10 cm or more on the scalp, neck, cheeks or in the periorbital area. In parallel, purulent meningitis, otitis media, pneumonia, etc. may occur.
Histological examination of the affected areas of the skin shows an inflammatory infiltrate, which consists of erythrocytes, leukocytes, histiocytes and lymphocytes. The diagnosis is confirmed by blood culture on culture media to isolate H. influenzae. Antibiotic therapy is carried out until the lesions disappear and the temperature returns to normal.
Acute epiglottitis is also known as inflammation of the epiglottis . This is a severe form of hemophilus influenzae infection in children aged 2 to 5 years. The disease begins acutely, the temperature rises quickly and strongly, and sharp pain in the throat appears. Symptoms such as severe shortness of breath, inability to swallow, narrowing or blockage of the larynx in the epiglottis area, resulting in respiratory distress, are also noted. In some cases, symptoms such as excessive salivation, aphonia, cyanosis, and pallor are observed. The patient's nasal wings swell.
Infants in the absence of meningeal symptoms often throw their heads back. In older children, examination of the oropharynx reveals a swollen red epiglottis. Also, the inflammatory process occurs in the subglottic space.
Epiglottitis is usually severe. Within a few hours, there is a risk of laryngeal obstruction, loss of consciousness, and death unless nasotraxal intubation or tracheotomy is promptly initiated.
Hemophilic pericarditis , according to American literature, accounts for about 15% of all cases of pericarditis in children. The symptoms of the disease are similar to pericarditis of other bacterial nature. Symptoms of hemophilic pericarditis in children: high body temperature, tachycardia, expansion of the boundaries of cardiac dullness, respiratory disorders, dullness of heart sounds. The disease is very severe and deaths are common.
Purulent arthritis. In our country, arthritis caused by H. influenza is extremely rare. The disease affects large joints: elbow, knee, shoulder, hip. The symptoms of this arthritis are similar to those of other bacterial etiologies.
Purulent arthritis in children can be combined with other diseases of hemophilic nature - cellulitis, purulent meningitis, etc. The final diagnosis requires blood cultures and intra-articular fluid, as well as examination of Gram-stained brains.
Osteomyelitis caused by N. influenzae is characterized by damage to large tubular bones: tibia, femur, humerus. For diagnosis, bacteriological cultures of bone marrow aspirate and Gram-stained smears are used.
In newborns, hemophilus influenzae infection is often generalized, with symptoms of septicemia or septicopyemia, and the occurrence of multiple lesions. There is a high percentage of death as a result of the disease, since the course is very severe.
Treatment
If there are no etiotropic therapeutic measures, this causes high mortality in patients with this diagnosis. Therapy requires immediate medical intervention and constant monitoring by medical personnel. Until the 1970s, treatment with ampicillin was most effective. But bacterial mutations have led to the pathogen acquiring extreme resistance and becoming resistant to this drug.
Therapy is recommended with the following drugs: cephalosporin, levomecithin and ampicillin. The fact of constant modifications and adaptability of the infection to antimicrobial medications has led to a decrease in the effectiveness of their use. But there are also the latest developments in this area, providing those affected with new medications that can act on current viral strains.
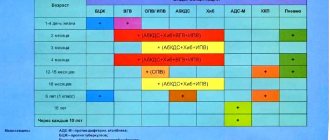
IMMUNIZATION SCHEME
Vaccination against Haemophilus influenzae is carried out in infancy in the absence of contraindications.
The vaccination schedule varies depending on the patient’s age group:
- The first vaccination against hemophilus influenzae is recommended for babies at 3 months. Vaccination is often combined with immunization against diphtheria, whooping cough and tetanus. The next 2 vaccinations are given at 4 and 6 months. Thanks to three doses of the vaccine, the child receives reliable immunity in 95% of cases. After revaccination at 1.5 years, almost 100% protection is formed;
- If vaccinations against hemophilus influenzae infection began after 6 months, then a double dose of the vaccine is sufficient. The interval between vaccinations is 1 month. Revaccination should be carried out 12 months after the last immunization. However, the vaccine is usually given at 1.5 years of age along with DPT;
- For children over 1 year old, it is enough to get 1 vaccination against Haemophilus influenzae. By this age, most babies are exposed to a pathogenic microbe, so they have managed to develop the necessary antibodies. Vaccination allows you to form reliable immunity against Haemophilus influenzae in case of re-infection.
This vaccination schedule allows 95% of vaccinated children to develop reliable immunity, which will last for up to 5 years. Adults are vaccinated against hemophilus influenzae once, because the body of such patients has the necessary antibodies.
Prevention
The modern vaccination calendar provides for vaccination against hemophilus influenzae. This vaccination is carried out for children from 3 months to five years. Children over five years old do not need such a procedure, since their immune system is able to independently fight the pathogen.
Vaccination is also carried out according to individual indications for persons with frequent acute respiratory viral infections, damage to the central nervous system, and indications for removal of the spleen (in this case, immunization is carried out before surgery).
Other preventive measures include identifying carriers in older people and prescribing adequate treatment for them, strengthening the immune system (balanced diet, taking multivitamins), etc.
WHEN IS IMMUNIZATION REQUIRED?
Vaccination against hemophilus influenzae is recommended for patients of the following categories:
- All infants who have reached 3 months of age;
- Organized children attending children's groups (sports sections, kindergartens, clubs);
- Patients of any age who have severe immunodeficiency (HIV, cancer);
- Elderly people;
- Patients after removal of the spleen;
- Children living in large families or orphanages;
- Infants who are bottle-fed. In such a situation, the child does not receive antibodies with milk, and therefore cannot resist infections;
- Frequently ill children;
- Babies who were born prematurely.
The peak development of meningitis and pneumonia caused by Haemophilus influenzae occurs at the age of 6-12 months. Therefore, it is necessary to get vaccinated against Haemophilus influenzae in a timely manner.
Vaccination of infants has been mandatory since 2011, the procedure is carried out in district clinics. For children over 1 year of age, immunization helps protect against other types of Haemophilus influenzae infection: acute respiratory infections, otitis media and bronchitis.
Causes of the disease
The causative agents of the purulent form of the disease are bacteria (streptococcal, staphylococcal infections, Haemophilus influenzae, etc.). In order for an inflammatory process to start in the maxillary sinus, the body must have favorable conditions for the reproduction and activation of bacterial flora. Such provoking factors contributing to the development of inflammation are:
- complicated colds and acute respiratory viral infections;
- mechanical injuries of the nose (fractures, bruises);
- chronic diseases of the nasopharynx (rhinitis, tonsillitis, adenoids);
- allergic rhinitis;
- carious teeth of the upper jaw;
- deviated nasal septum;
- the presence of cysts, polyps and other formations in the nose;
- hypothermia;
- poor working conditions (working in “harmful” industries, when a person is constantly in contact with dust and toxic substances);
- poor hygiene of the nasal cavity at the onset of an infectious disease.
If the cause of purulent sinusitis is correctly identified and eliminated, treatment of inflammation will be more effective.
Causes and mechanism of development of adenoids in children
The formation of the tonsils is subject to various influences during the first 5-7 years of life. It is also worth noting that young children have insufficiently developed immunity. As a result, various factors (genetic, infectious, environmental) lead to disruptions in the immune system - the development of an immunodeficiency state.
An important role in the formation of adenoids in children is played by:
- Strepto- and staphylococci
- Haemophilus influenzae
- Chlamydia, mycoplasma
- Adenovirus infection
- Fungal infection
Against the background of immunodeficiency, these microorganisms lead to constant irritation of the tonsil, which ultimately leads to its enlargement and proliferation. In addition to the indicated mechanism for the development of the disease, there are others:
- Development of lymphaticism. Lymphatism is a predisposition of a small organism to hereditary deficiency of the lymphoid system. In this case, the adenoids will be an integral part of this pathology.
- Allergy . Allergy also plays a certain role in the development of adenoids. The same microorganisms, as well as food allergens, act as allergenic factors.