Pharmacodynamics and pharmacokinetics
What is Ceftriaxone?
According to Wikipedia, ceftriaxone is an antibiotic whose bactericidal effect is due to its ability to disrupt the synthesis of peptidoglycan in bacterial cell walls.
Pharmacodynamics
A universal antibacterial agent, the mechanism of action of which is determined by the ability to suppress the synthesis of the bacterial cell wall. The drug exhibits greater resistance to most β-lactamases of gram(+) and gram(-) microorganisms.
Active regarding:
- Gram(+) aerobes - St. aureus (including penicillinase-producing strains) and Epidermidis, Streptococcus (pneumoniae, pyogenes, viridans group);
- Gram(-) aerobes - Enterobacter aerogenes and cloacae, Acinetobacter calcoaceticus, Haemophilus influenzae (including penicillinase-producing strains) and parainfluenzae, Borrelia burgdorferi, Klebsiella spp. (including pneumoniae), Escherichia coli, Moraxella catarrhalis and diplococci of the genus Neisseria (including penicillinase-producing strains), Morganella morganii, Proteus vulgaris and Proteus mirabilis, Neisseria meningitidis, Serratia spp., some strains of Pseudomonas aeruginosa;
- anaerobes - Clostridium spp. (exception: Clostridium difficile), Bacteroides fragilis, Peptostreptococcus spp..
In vitro (clinical significance remains unknown) activity is observed against strains of the following bacteria: Citrobacter diversus and freundii, Salmonella spp. (including against Salmonella typhi), Providencia spp. (including in relation to Providencia rettgeri), Shigella spp.; Bacteroides bivius, Streptococcus agalactiae, Bacteroides melaninogenicus.
Methicillin -resistant Staphylococcus, many strains of Enterococcus (including Str. faecalis) and group D Streptococcus are resistant to cephalosporin antibiotics (including ceftriaxone).
Pharmacokinetics
- bioavailability - 100%;
- T Cmax when Ceftriaxone is administered intravenously - at the end of the infusion, when administered intramuscularly - 2-3 hours;
- connection with plasma proteins - from 83 to 96%;
- T1/2 with intramuscular administration - from 5.8 to 8.7 hours, with intravenous administration - from 4.3 to 15.7 hours (depending on the disease, the patient’s age and the condition of his kidneys).
In adults, the concentration of ceftriaxone in the cerebrospinal fluid when administered 50 mg/kg after 2-24 hours is many times higher than the MIC (minimum inhibitory concentration) for the most common pathogens of meningococcal infection . The drug penetrates well into the cerebrospinal fluid during inflammation of the meninges.
Ceftriaxone is excreted unchanged:
- kidneys - by 33-67% (in newborn babies this figure is 70%);
- with bile into the intestines (where the drug is inactivated) - by 40-50%.
Hemodialysis is ineffective.
Indications for use of Ceftriaxone
The annotation states that the indications for the use of Ceftriaxone are infections caused by bacteria sensitive to the drug. Intravenous infusions and injections of medications are prescribed to treat:
- infections of the abdominal cavity (including empyema of the gallbladder , angiocholitis , peritonitis ), ENT organs and respiratory tract ( empyema of the pleura , pneumonia , bronchitis , lung abscess , etc.), bone and joint tissue, soft tissues and skin, urogenital tract (including pyelonephritis , pyelitis , prostatitis , cystitis , epididymitis );
- epiglottitis;
- infected burns/wounds;
- infectious lesions of the maxillofacial area;
- bacterial septicemia;
- sepsis;
- bacterial endocarditis;
- bacterial meningitis;
- syphilis;
- chancroid;
- tick-borne borreliosis (Lyme disease);
- uncomplicated gonorrhea (including in cases where the disease is caused by microorganisms that secrete penicillinase);
- salmonellosis/salmonella carriage;
- typhoid fever.
The drug is also used for perioperative prophylaxis and for the treatment of immunocompromised patients.
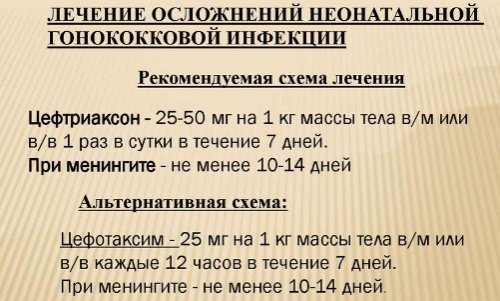
What is Ceftriaxone used for for syphilis?
Although Penicillin is the drug of choice of syphilis , its effectiveness may be limited in some cases.
The use of cephalosporin antibiotics is resorted to as a backup option in case of intolerance to drugs of the penicillin group.
The valuable properties of the drug are:
- the presence in its composition of chemical substances that have the ability to suppress the formation of cell membranes and mucopeptide synthesis in the walls of bacterial cells;
- the ability to quickly penetrate organs, fluids and tissues of the body and, in particular, into the cerebrospinal fluid, which in patients with syphilis undergoes many specific changes;
- Possibility of use for the treatment of pregnant women.
The medicine is most effective in cases where the causative agent of the disease is Treponema pallidum, since the distinctive feature of Ceftriaxone is its high treponemocidal activity. The positive effect is especially pronounced with intramuscular administration of the drug.
Treatment of syphilis with the use of the drug gives good results not only in the early stages of the disease, but also in advanced cases: with neurosyphilis , as well as with secondary and latent syphilis.
Since T1/2 of Ceftriaxone is approximately 8 hours, the drug can be used equally successfully in both inpatient and outpatient treatment regimens. It is enough to administer the drug to the patient once a day.
For preventive treatment, the drug is administered over 5 days, for primary syphilis - a 10-day course, early latent and secondary syphilis are treated within 3 weeks.
For non-advanced forms of neurosyphilis, the patient is administered a single dose of 1-2 g of Ceftriaxone for 20 days; in the later stages of the disease, the drug is administered at a dose of 1 g/day. for 3 weeks, after which an interval of 14 days is maintained and treatment with a similar dosage is carried out for 10 days.
For acute generalized meningitis and syphilitic meningoencephalitis, the dose is increased to 5 g/day.
Ceftriaxone injections: why is the drug prescribed for angina in adults and children?
Despite the fact that the antibiotic is effective for various lesions of the nasopharynx (including sore throat and sinusitis ), it is, as a rule, rarely used as a drug of choice, especially in pediatrics.
For angina, the medicine can be administered through a dropper into a vein or in the form of regular injections into the muscle. However, in the vast majority of cases, the patient is prescribed intramuscular injections. The solution is prepared immediately before use. The finished mixture remains stable at room temperature for 6 hours after preparation.
For children with angina, Ceftriaxone is prescribed in exceptional cases when acute angina is complicated by severe suppuration and inflammation.
The appropriate dosage is determined by the attending physician.
During pregnancy, the drug is prescribed in cases where penicillin antibiotics are not effective. Although the medicine crosses the placental barrier, it does not have a significant effect on the health and development of the fetus.
Treatment of sinusitis with Ceftriaxone
For sinusitis, antibacterial agents are first-line drugs. Completely penetrating the blood, Ceftriaxone is retained at the site of inflammation in the required concentrations.
As a rule, the medicine is prescribed in combination with mucolytics , vasoconstrictors , etc.
How to inject the drug for sinusitis? Typically, the patient is prescribed Ceftriaxone to be injected into the muscle twice a day, 0.5-1 g. Before injection, the powder is mixed with Lidocaine (it is preferable to use a one percent solution) or d/i water.
Treatment lasts at least 1 week.
Negative sides
In modern society, there is a stereotype that treatment with injections is much more productive and will give the desired result faster, however, in most cases this is not the case. Nowadays there are enough drugs used orally, which are in no way inferior to treatment with injections. I would like to draw attention to the disadvantages of using the injection method.
- Everything related to injections causes hostility, pain, and fear.
- If sterility is violated, an infection transmitted only through blood, for example, viral hepatitis B and AIDS, can be introduced into the body.
- Complications can be caused by incorrect insertion; the needle may accidentally hit a nerve, which can lead to complex consequences.
- There are cases when, after the injection, the tissue at the injection site turns red, becomes painful, and in the worst case, an abscess may occur that will need to be opened.
- When given an injection, allergic reactions are more acute than when using the same drug orally in capsules or tablets. When administering injections, the possibility of anaphylactic shock is several times higher than in other cases.
Experts around the world strive to limit the number of injections . The best pharmacologists from leading companies see their task as creating drugs that act quickly and effectively when taken orally. It is unlikely that it will be possible to completely abandon injections, especially when treating emergency conditions, but minimizing the number and limiting the indications is a completely feasible task.
Positive sides
- Injections are effective in cases where rapid penetration of the drug into the blood and an immediate therapeutic effect are necessary.
- Injections are used when the drug cannot be administered through the oral cavity, as it will be destroyed in the gastrointestinal tract.
- It is impossible to drink the medication, for example, if you are unconscious or vomiting.
- The drug used, when administered by syringe, has a more pronounced and longer-lasting effect.
Technical side
Everyone in their life has been faced with the need to give themselves or loved ones a simple intramuscular injection. It's quite simple if you know how to do it and don't be afraid. The recommendations written below apply specifically to intramuscular injections, but it is better to entrust intravenous injections to people with medical education and not risk doing it yourself.
- Be sure to wash your hands with soap.
- Next, check the expiration date of the drug that needs to be administered.
- Taking the ampoule, shake it, lightly tap the tip with your fingernail so that no liquid remains in it, wipe the tip with a cotton swab moistened with alcohol.
- Then you need to open the ampoule with the medicine; to do this, remove the ampoule file from the cardboard box with the medicine. Taking the file, run it forcefully along the base of the tip several times, and then carefully break it off.
- Unpack the syringe without removing the cap from the needle and put it on the syringe.
- Carefully, without touching the needle, remove the plastic cap from it and draw up the medicine.
- Turn the syringe vertically up, and, holding it in this light position, tap it with your fingernail so that the air bubbles rise to the top.
- Press lightly to release air from the syringe; when a drop of medicine appears at the tip of the needle, stop.
- Place a cap on the needle.
- Place the patient on their stomach or side to relax the butt muscles.
- Mentally divide the buttock into four squares, the injection is made in the upper outer square.
- The place where the injection will be given must be wiped with a cotton swab dipped in an alcohol solution.
- To reduce pain, the skin at the injection site can be stretched or squeezed with the fingers of the other hand. In children, the skin should not be stretched under any circumstances; it should be compressed.
- With a sharp movement at a right angle, insert the needle 3/4 of the way through, that is, almost to the very end.
- Gradually, slowly, introduce the medicine.
- With a sharp movement, remove the needle and press the injection site with cotton wool moistened with alcohol.
- Massage the affected muscle.
If possible, limit the number of injections in one place; it is advisable not to inject in one area more than 2 times a week. To do this, alternate sides: on the first day, inject into the right side, on the second, into the left.
In addition, you may encounter the fact that the injection medicine is in powder form. In this case, you need to dilute it with special distilled water or novocaine in ampoules. To dilute the medicine you will need one syringe and two needles.
How to properly dilute powdered medicine
- Take an ampoule with liquid, it can be distilled water or novocaine, and use a needle to draw it into a syringe;
- Wipe the lid of the bottle with the powder with a cotton swab and alcohol and inject liquid from the syringe into it;
- Remove the syringe and shake the bottle well until the powder is completely dissolved;
- Then, draw the solution into the syringe again;
- Place a new needle on the syringe without removing the cap.
- The solution for administration is ready.
Contraindications
Ceftriaxone is not prescribed in case of known hypersensitivity to cephalosporin antibiotics or auxiliary components of the drug.
Relative contraindications:
- the neonatal period if the child has hyperbilirubinemia ;
- prematurity;
- renal/liver failure;
- enteritis , UC or colitis associated with the use of antibacterial agents;
- pregnancy;
- lactation.
Side effects of Ceftriaxone
Side effects of the drug appear as:
- hypersensitivity reactions: eosinophilia , fever, itching, urticaria edema , skin rash, multiforme (in some cases malignant) exudative erythema , serum sickness , anaphylactic shock , chills;
- headache and dizziness;
- oliguria;
- dysfunction of the digestive organs: nausea, vomiting, flatulence , taste disturbance, stomatitis , diarrhea , glossitis , formation of sludge in the gallbladder and pseudocholelithiasis , pseudomembranous enterocolitis , dysbacteriosis , candidomycosis and other superinfections;
- hematopoiesis disorders: anemia (including hemolytic ), lymphopenia , leukopenia, neutropenia, thrombocytopenia, granulocytopenia , thrombocytosis and leukocytosis , hematuria , basophilia , nosebleeds).
If the medicine is administered intravenously, inflammation of the venous wall, as well as pain along the vein, is possible. The injection of the drug into the muscle is accompanied by pain at the injection site.
Ceftriaxone (injections and IV infusion) may also affect laboratory parameters. The patient's prothrombin time decreases (or increases), the activity of alkaline phosphatase and liver transaminases increases, as well as the concentration of urea, hypercreatininemia , hyperbilirubinemia , and glycosuria .
Reviews of the side effects of Ceftriaxone allow us to conclude that with intramuscular administration of the drug, almost 100% of patients complain of severe pain from the injection, some report muscle pain, dizziness, chills, weakness, itching and rash.
The injections are easiest to tolerate if you dilute the powder with an anesthetic. In this case, it is necessary to do a test both for the drug itself and for the painkiller.
How to dissolve Ceftriaxone with Procaine
Before taking Procaine as a solvent, you need to find out whether there are any contraindications to the use of Novocaine.
If the patient has increased susceptibility to Novocaine, then its use can provoke anaphylactic shock. Therefore, 0.5 ml of liquid product is injected into the muscle. If after half an hour there are no changes, then you can inject the rest of the dose, only into the other buttock.
Solutions must be prepared immediately before use.
Because of:
- the antibiotic in a dissolved state remains stable for only six hours;
- stale solution can increase pain symptoms. Freshly prepared liquid is used once.
How to dilute Ceftriaxone with Novocaine, what is needed for this?
- To prepare a solution with Novocaine, you need to add 5 ml of Novocaine to a syringe for 1 g of Ceftriaxone. With a smaller quantity, the powder content of the bottle will not completely dissolve. The syringe, or rather the needle, will become clogged with undissolved lumps.
- Then the syringe with the solvent is injected into the bottle with the powder. Shake the contents well without removing the corner. The diluted drug is ready for use.
- After dilution, as much liquid medicine as required is drawn into the syringe. The rest is thrown away.
The instructions for use indicate Lidocaine as the agent that is recommended for diluting the powdered drug. But the use of special water for injection is allowed, as well as Procaine.
Instructions for use of Ceftriaxone (Method and dosage)
How to dilute Ceftriaxone for injection?
The manufacturer's instructions, as well as the Vidal reference book, indicate that the drug can be injected into a vein or into a muscle.
Dosage for adults and children over 12 years of age: 1-2 g/day. The antibiotic is administered once or once every 12 hours at half the dose.
In particularly serious cases, as well as if the infection is caused by a pathogen moderately sensitive to Ceftriaxone, the dose is increased to 4 g/day.
For gonorrhea , a single injection of 250 mg of the drug into the muscle is recommended.
For preventive purposes, before an infected or suspected infected operation, depending on the degree of danger of infectious complications, the patient should be administered a single dose of 1-2 g of Ceftriaxone 0.5-1.5 hours before surgery.
For children in the first 2 weeks of life, the medicine is administered 1 time per day. The dose is calculated using the formula 20-50 mg/kg/day. The highest dose is 50 mg/kg (which is due to the underdevelopment of the enzyme system).
The optimal dosage for children under 12 years of age (including infants) is also selected depending on weight. The daily dose varies from 20 to 75 mg/kg. For children weighing more than 50 kg, Ceftriaxone is prescribed in the same dose as for adults.
Doses greater than 50 mg/kg should be administered as an intravenous infusion over at least 30 minutes.
For bacterial meningitis, treatment begins with a single dose of 100 mg/kg/day. The highest dose is 4 g. As soon as the pathogen is isolated and its sensitivity to the drug is determined, the dose is reduced.
Reviews about the drug (in particular, about its use in children) allow us to conclude that the drug is very effective and affordable, but its significant drawback is severe pain at the injection site. As for side effects, according to the patients themselves, there are no more of them than with any other antibiotic.
How many days to inject the drug?
The duration of treatment depends on what pathogenic microflora causes the disease, as well as on the characteristics of the clinical picture. If the causative agent is Gram (-) diplococci of the genus Neisseria, the best results can be achieved in 4 days, if enterobacteria are sensitive to the drug - in 10-14 days.
Ceftriaxone injections, instructions for use. How to dilute the drug?
Lidocaine solution (1 or 2%) or water for injection (d/i).
When using water d/i, it should be taken into account that intramuscular injections of the drug are very painful, so if the solvent is water, there will be discomfort both during the injection and for some time after it.
Water for diluting the powder is usually taken in cases where the use of Lidocaine is impossible due to the patient being allergic to it.
The best option is a one percent solution of Lidocaine. It is better to use water as an adjuvant when diluting the drug with Lidocaine 2%.
Is it possible to dilute Novocaine with Ceftriaxone?
Novocaine , when used to dilute the drug, reduces the activity of the antibiotic, while at the same time increasing the likelihood of the patient developing anaphylactic shock .
Based on the reviews of the patients themselves, they note that Lidocaine is better than Novocaine in relieving pain when Ceftriaxone is administered.
In addition, the use of a non-freshly prepared solution of Ceftriaxone with Novocaine increases pain during injection (the solution remains stable for 6 hours after preparation).
How to dilute Ceftriaxone with Novocaine?
If Novocain is used as a solvent, it is taken in a volume of 5 ml per 1 g of the drug. If you take a smaller amount of Novocaine, the powder may not completely dissolve, and the syringe needle will become clogged with lumps of medicine.
Dilution with Lidocaine 1%
For injection into the muscle, 0.5 g of the drug is dissolved in 2 ml of a one percent solution of Lidocaine (the contents of one ampoule); For 1 g of the drug take 3.6 ml of solvent.
The dosage of 0.25 g is diluted in the same way as 0.5 g, that is, with the contents of 1 ampoule of 1% Lidocaine. After this, the finished solution is drawn into different syringes, half the volume in each.
The medicine is injected deep into the gluteal muscle (no more than 1 g in each buttock).
The drug diluted with Lidocaine is not intended for intravenous administration. It is allowed to be injected strictly into the muscle.
How to dilute Ceftriaxone injections with Lidocaine 2%?
To dilute 1 g of the drug, take 1.8 ml of water and two percent Lidocaine. To dilute 0.5 g of the drug, also mix 1.8 ml of Lidocaine with 1.8 ml of water, but only half of the resulting solution (1.8 ml) is used for dissolution. To dilute 0.25 g of the drug, take 0.9 ml of a solvent prepared in a similar way.
How to dilute Ceftriaxone for intramuscular administration in children?
This method of intramuscular injection is practically not used in pediatric practice, since Ceftriaxone with Novocaine can cause severe anaphylactic shock in a child, and in combination with Lidocaine, it can contribute to the occurrence of convulsions and disruption of the heart.
For this reason, the optimal solvent when using the drug in children is ordinary water. The impossibility of using painkillers in childhood requires an even slower and more careful administration of the medicine in order to reduce pain during the injection.
Dilution for intravenous administration
For intravenous administration, 1 g of the drug is dissolved in 10 ml of distilled water (sterile). The drug is administered slowly over 2-4 minutes.
Dilution for intravenous infusion
When carrying out infusion therapy, the drug is administered for at least half an hour. To prepare a solution, 2 g of powder is diluted in 40 ml of a Ca-free solution: dextrose (5 or 10%), NaCl (0.9%), fructose (5%).
Additionally
Ceftriaxone is intended exclusively for parenteral administration: manufacturers do not produce tablets and suspensions due to the fact that the antibiotic, when in contact with body tissues, is highly active and severely irritates them.
Doses for animals
The dosage for cats and dogs is selected taking into account the body weight of the animal. As a rule, it is 30-50 mg/kg.
If a 0.5 g bottle is used, 1 ml of two percent Lidocaine and 1 ml of water d/i (or 2 ml of Lidocaine 1%) should be added to it. After vigorously shaking the medicine until the lumps are completely dissolved, it is drawn into a syringe and injected into the muscle or under the skin of the sick animal.
The dosage for a cat (Ceftriaxone 0.5 g is usually used for small animals - cats, kittens, etc.), if the doctor prescribed 40 mg of Ceftriaxone per 1 kg of weight, is 0.16 ml/kg.
For dogs (and other large animals), take bottles of 1 g. The solvent is taken in a volume of 4 ml (2 ml Lidocaine 2% + 2 ml water for injection). For a dog weighing 10 kg, if the dose is 40 mg/kg, you need to administer 1.6 ml of the prepared solution.
If it is necessary to administer Ceftriaxone intravenously through a catheter, sterile distilled water is used for dilution.
Methods of drug administration
The medication is administered in two ways: into a vein or into muscle fibers. Doctors choose an option depending on the disease and the patient’s condition. The effect appears much faster when the medicine is injected into a vein.
The medicine is diluted in different ways:
- lidocaine;

- novocaine;
- water for injections.
Lidocaine is usually used when the drug is administered through a muscle. An anesthetic substance reduces the pain from the injection. When a medication is injected into a vein, it is diluted with saline solution. This method is used if the patient has allergies. The water must be sterile. This is necessary to prevent the penetration of a secondary infection that is resistant to the substance used.
Doctors themselves determine the treatment method, based on the pathogen and the characteristics of the pathology:
- For gonorrhea, 250 g of the drug is prescribed. The injection is performed inside the muscle. The drug is administered once.
- To cure meningitis, the drug is calculated as follows: per 1 kg. 100 mg. medications. More than 4 g should not be prescribed.
- When a positive effect is observed, the dose is reduced. For prophylaxis or before an upcoming operation, 1 - 2 g of the drug is administered.
When the baby turns 14 days old, he can be administered the medication once a day. The dose is calculated as follows: per 1 kg. 20 - 50 mg. Do not use more than 50 mg per day.
For patients under 12 years of age, the dose is determined by weight. The amount of medicine can increase to 75 mg. When a small patient weighs more than 50 kg, he is prescribed the usual dosage. If more than 50 mg/kg is required, administer intravenously. Pour in slowly using a dropper. The procedure lasts from 30 minutes. In this case, the medication is diluted with saline solution.

Typically, lidocaine is used to dilute the drug with water for injections. Divide the composition into 2 parts. The prepared mixture can be stored for no longer than 6 hours.
Children are prohibited from diluting the medication with anesthetics, so as not to cause convulsions and anaphylaxis.
Children are prescribed only Ceftriaxone with water for injection, distilled liquid. The medicine is administered very slowly. This allows the baby to experience a minimum of discomfort. For 1 g of medication take 10 ml.
To give injections to adult patients inside the muscle fibers, use a 4-cc needle. An injection is given in the buttock. The needle is not inserted to the level of the dermis by 2 - 3 mm. More than 1 g of medication is not injected into the muscles.
Interaction
In one volume, it is pharmaceutically incompatible with other antimicrobial agents.
By suppressing intestinal microflora, it prevents the formation of vitamin K . For this reason, the use of the drug in combination with drugs that reduce platelet aggregation (sulfinpyrazone, NSAIDs) may provoke bleeding.
The same feature of Ceftriaxone enhances the effect of anticoagulants when used together.
In combination with loop diuretics, the risk of nephrotoxicity increases.
special instructions
The drug is used in a hospital setting. In patients who are on hemodialysis, as well as with simultaneous severe hepatic and renal failure, plasma concentrations of Ceftriaxone should be kept under control.
With long-term treatment, regular monitoring of the peripheral blood picture and indicators characterizing the function of the kidneys and liver is required.
Sometimes (rarely) an ultrasound of the gallbladder may show shadows that indicate the presence of sediment. The darkening disappears after stopping the course of treatment.
vitamin K in addition to Ceftriaxone .
If there is an imbalance of water and electrolytes, as well as arterial hypertension , the level of sodium in the blood plasma should be monitored. If the treatment is long-term, the patient is advised to undergo a general blood test.
Like other cephalosporins, the drug has the ability to displace bilirubin , and therefore it is used with caution in newborns with hyperbilirubinemia (and, in particular, in premature infants).
The drug does not affect the speed of neuromuscular conduction.
Ceftriaxone
Hypersensitivity reactions
As with other β-lactam antibiotics, severe hypersensitivity reactions, some fatal, have been reported. If a severe hypersensitivity reaction develops, ceftriaxone therapy should be discontinued immediately and appropriate emergency treatment measures taken. Before starting therapy with ceftriaxone, it is necessary to determine whether the patient has had hypersensitivity reactions to ceftriaxone, cephalosporins or severe hypersensitivity reactions to other β-lactam antibiotics (penicillins, monobactams and carbapenems).
Caution should be exercised when using ceftriaxone in patients with a history of mild hypersensitivity reactions to other β-lactam antibiotics (penicillins, monobactams and carbapenems).
Sodium content
1.0 g of Ceftriaxone contains 3.6 mmol of sodium. This should be taken into account in patients on a sodium controlled diet.
Hemolytic anemia
As with the use of other cephalosporins, autoimmune hemolytic anemia may develop during treatment with Ceftriaxone. Cases of severe hemolytic anemia have been reported in adults and children, including deaths.
If anemia develops in a patient being treated with ceftriaxone, the diagnosis of cephalosporin-associated anemia cannot be excluded and treatment must be discontinued until the cause is determined.
Diarrhea caused by Clostridium difficile
As with the use of most other antibacterial drugs, cases of diarrhea caused by Clostridium difficile (C. difficile) have been reported during treatment with ceftriaxone.
varying severity: from mild diarrhea to fatal colitis.
Treatment with antibacterial drugs suppresses the normal microflora of the colon and provokes the growth of C. difficile
.
In turn, C. difficile
produces toxins A and B, which are factors in the pathogenesis of diarrhea caused by
C. difficile.
strains
of C. difficile
are infectious agents with a high risk of morbidity and mortality due to possible resistance to antimicrobial therapy, and treatment may require colectomy.
C. difficile
diarrhea in all patients with diarrhea after antibiotic therapy.
A thorough medical history is necessary, since there have been cases of diarrhea caused by C. difficile
more than 2 months after antibiotic therapy.
C. difficile
diarrhea is suspected or confirmed current non-
C. difficile
antibiotic therapy may need to be discontinued.
In accordance with clinical indications, appropriate treatment should be prescribed with the administration of fluids and electrolytes, proteins, antibiotic therapy for C. difficile
, and surgical treatment. Do not use medications that inhibit intestinal motility.
Superinfections
As with treatment with other antibacterial drugs, superinfections may develop.
Changes in prothrombin time
Rare cases of changes in prothrombin time have been described in patients receiving ceftriaxone. Patients with vitamin K deficiency (impaired synthesis, malnutrition) may require monitoring of prothrombin time during therapy and administration of vitamin K (10 mg/week) if the prothrombin time increases before or during therapy.
Formation of precipitates of ceftriaxone calcium salt
Cases of fatal reactions resulting from the deposition of ceftriaxone-calcium precipitates in the lungs and kidneys of newborns have been described. Theoretically, there is a possibility of interaction of ceftriaxone with calcium-containing solutions for intravenous administration in other age groups of patients, therefore ceftriaxone should not be mixed with calcium-containing solutions (including for parenteral nutrition), and also administered simultaneously, including through separate access for infusions at different areas. Theoretically, based on the calculation of the 5 half-lives of ceftriaxone, the interval between the administration of ceftriaxone and calcium-containing solutions should be at least 48 hours.
There are no data on the possible interaction of ceftriaxone with calcium-containing drugs for oral administration, as well as ceftriaxone for intramuscular administration with potassium-containing drugs (intravenously or orally).
After using ceftriaxone, usually in doses exceeding the standard recommended (1.0 g per day or more), ultrasound examination of the gallbladder revealed precipitates of the calcium salt of ceftriaxone, the formation of which is most likely in pediatric patients. Precipitates rarely cause any symptoms and disappear after completion or cessation of ceftriaxone therapy. If these phenomena are accompanied by clinical symptoms, conservative non-surgical treatment is recommended, and the decision to discontinue the drug is left to the discretion of the attending physician and should be based on an individual assessment of benefit and risk.
Although there is evidence of the formation of intravascular precipitates only in neonates when using ceftriaxone and calcium-containing infusion solutions or any other calcium-containing drugs, Ceftriaxone should not be mixed or prescribed to children and adult patients simultaneously with calcium-containing infusion solutions, even using different venous approaches (see sections “Contraindications”, “Interaction with other drugs”).
Pancreatitis
Rare cases of pancreatitis, possibly due to bile duct obstruction, have been described in patients receiving ceftriaxone. Most of these patients had preexisting risk factors for biliary congestion, such as prior therapy, severe illness, and total parenteral nutrition. At the same time, it is impossible to exclude the triggering role in the development of pancreatitis of precipitates formed under the influence of ceftriaxone in the biliary tract.
Use in children
The safety and effectiveness of ceftriaxone in neonates, infants, and young children have been determined at the dosages described in the Dosage and Administration section. Studies have shown that, like other cephalosporins, ceftriaxone can displace bilirubin from binding to serum albumin. Ceftriaxone should not be used in newborns, especially premature infants, who are at risk of developing bilirubin encephalopathy (see section "Contraindications").
Long-term treatment
With long-term treatment, it is necessary to regularly monitor the peripheral blood picture, indicators of the functional state of the liver and kidneys.
Blood test monitoring
During long-term treatment, a complete blood count should be performed regularly.
Serological studies
When treated with ceftriaxone, false-positive results of the Coombs test, galactosemia test, and determination of glucose in urine may be observed (it is recommended to determine glucosuria only by the enzyme method).
Ceftriaxone analogues, what can replace the drug?
Level 4 ATC code matches:
Cephosin
Lendatsin
Medakson
Loprax
Cefixime
Lorakson
Sulperazon
Cefoperazone
Rocephin
Tsedex
Fortum
Ceftazidime
Cefotaxime
Cefix
Ceforal Solutab
Pantsef
Claforan
Cefodox
Suprax Solutab
Analogues of Ceftriaxone in injections:
- Ceftriaxone-LEKSVM (Kabi, Jodas, KMP, Promed, Vial, Elfa)
- Ceftriabol
- Tsefson
- Cefaxon
- Torotsef
- Hizon
- Cephogram
- Medakson
- Lorakson
- Ifitsef
Analogues in tablets:
- Pantsef
- Suprax Solutab
- Ceforal Solutab
- Cefpotec
- Spectraceph
Ceftriaxone or Cefazolin - which is better?
Both drugs belong to the cephalosporin group, but Ceftriaxone is a third-generation antibiotic, and Cefazolin is a first-generation drug.
An important feature of first generation cephalosporin antibiotics is that they are not effective against listeria and enterococci, have a narrow spectrum of action and a low level of activity against gram(-) bacteria.
Cefazolin is used mainly in surgery for perioperative prophylaxis, as well as for the treatment of soft tissue and skin infections.
Its prescription for the treatment of infections of the genitourinary system and respiratory tract cannot be considered as justified, which is associated with a narrow spectrum of antimicrobial activity and high resistance to it among potential pathogens.
Which is better: Ceftriaxone or Cefotaxime?
Cefotaxime and Ceftriaxone are the basic antimicrobial agents of the third generation cephalosporin group. The drugs are almost identical in their bactericidal properties.
Filippova Kira Alexandrovna
Plastic surgeon, dermatovenerologist, cosmetologist, Moscow
The fear of pain is stronger than the pain itself
The fears of doctors and their patients sometimes, albeit indirectly, coincide.
A patient, when visiting a cosmetologist’s office for the first time, almost always experiences fear of the unknown. Having not encountered such a procedure before, he is afraid of everything at once: the unnatural result, unwanted reactions that he read about on the Internet, long-term rehabilitation and, of course, pain.
Many patients, knowing their pain threshold, do not decide to undergo any injection procedure for years. The fear of pain is stronger than pain itself, British scientists found, whose article was published in the journal PLOS Computational Biology in 2013 [1]. The participants in their study were 30 people, some of whom suffered from chronic pain, and the rest from the consequences of their injuries. In particular, scientists were able to find out that the expectation of pain causes people suffering that is much stronger than that caused by the pain itself. All participants in the trial agreed to undergo a series of electric shocks for financial reward. At the same time, they were asked to choose one of two strike options that differed in strength. It turned out that all participants preferred a severe test if it had to come faster than a less painful blow.
So, fear of pain causes people suffering that is significantly stronger than what pain itself causes. Moreover, the identified pattern reaches its peak 15 minutes before the onset of pain. It is not yet completely clear how this feature of the human psyche affects the development of various disorders, phobias and manias. However, experts believe that further study of "expectation of pain" will help psychiatrists better understand the problems of their patients.
The main fear of a cosmetologist is the occurrence of an unwanted reaction or complication during and after the procedure. Naturally, each injection method has certain risks (ischemia, compression, migration, inflammation, etc.), therefore specialists try to use atraumatic injection instruments, proven drugs that, if necessary, can be removed from the skin tissue, and also regularly improve their skills at dissection courses .
Almost any procedure involving damage to the skin is, in one way or another, accompanied by a stage of pain relief. And here the question naturally arises about the possible occurrence of allergic reactions to the anesthetic. Let's figure out how great the risks are and whether the refusal of anesthesia by some doctors is justified.
Anesthesia. What to choose?
The main parameters of local anesthetics that determine their use include:
- strength and duration of action;
- safety (allergenicity, toxicity).
These parameters depend on the chemical structure of the active substances. Based on their chemical structure, the anesthetics currently used belong to one of two groups:
- esters:
- benzoic acid esters (cocaine, bencaine);
- esters of para-aminobenzoic acid (novocaine);
- esters of aminobenzoic and benzoic acids (dicaine);
- amides:
- amides of heterocyclic and aromatic acids (sovcaine, novocainamide);
- amides of aromatic amines - anilides ( lidocaine , bupivacaine, mepivacaine).
Strength and duration of action
Depending on the strength and duration of exposure, the following drugs are distinguished:
- with low activity and short action - procaine;
- with moderate activity and average duration of action - prilocaine, mepivacaine, lidocaine ;
- with high activity and long-lasting action - etidocaine, bupivacaine, tetracaine.
The effect of the drug is the result of contact with nerve fibers in situ. Local anesthetics block unmyelinated and thin myelinated fibers more easily and quickly. The degree to which sensitivity is turned off depends on the concentration of the local anesthetic, while the conduction of the impulses itself is blocked sequentially:
- temperature;
- painful;
- tactile;
- proprioceptive;
- motor;
- muscle relaxation.
The action of lidocaine is due to the stabilization of the neuronal membrane by reducing its permeability to sodium ions, which prevents the occurrence of an action potential and the conduction of nerve impulses. Lidocaine is effective for all types of local anesthesia: it inhibits the conduction of not only pain impulses, but also impulses of other modalities [2].
The degree and duration of the anesthetic effect of a local anesthetic is determined by its individual properties and some external factors, such as:
- acidity of the environment;
- anesthetic dissociation constant;
- lipophilicity of the anesthetic;
- percentage and rate of binding to plasma proteins.
The amount of anesthetic molecules entering neurons is regulated by the acidity of the tissue at the injection site. Local anesthetics are weak bases. For clinical use, they are usually available in the form of salts, as this improves the solubility and stability of the drugs. In order for the drug to exert its local anesthetic effect, hydrolysis of the salt and release of the base must occur. This process occurs only in an alkaline environment (tissue pH under normal conditions is 7.35–7.4), therefore, in inflamed tissues, local anesthetics are inactive, since in an acidic environment (pH at the site of inflammation is 5–6) hydrolysis of salts does not occur , and the base necessary for the specific effect is not released. The resulting bases penetrate the membrane of the nerve fiber (see figure).
Lidocaine quickly hydrolyzes in the slightly alkaline environment of tissues and, after a short latent period, acts for 1–1.5 hours. The anesthetic effect of lidocaine is 2–6 times stronger than procaine.
The dissociation constant of a drug reflects the proportion of ionized and non-ionized forms. A lower value of the constant determines the rapid onset of action, since more neutral molecules are formed. For example, lidocaine has the smallest constant, so its effect is considered the fastest, the effect of bupivacaine is medium, and procaine is slow.
The lipophilicity of bupivacaine and tetracaine gives them high activity and long-lasting action.
The degree of protein binding determines the duration of action and activity. Bupivacaine is bound to proteins by 90–97%, lidocaine by 60–75%, procaine by 0–6%.
The degree of binding of lidocaine to proteins largely depends on its concentration and the content of alpha-1-acid glycoprotein in the blood plasma. High protein binding may reduce the effect of free lidocaine or cause an overall increase in drug plasma concentrations. The therapeutic effect develops at a concentration of 1.5–5 μg/ml.
Safety
The allergenicity of the anesthetic is associated with its chemical nature. Anesthetics from the group of aromatic acid esters (novocaine, etc.) have the most pronounced anaphylactogenic properties. Local anesthetics of the amide group (lidocaine, trimecaine, bupivacaine) cause anaphylactic reactions much less frequently.
Lidocaine, when applied topically, dilates blood vessels, but does not have a locally irritating effect. Lidocaine can cause blurred vision, tremors, convulsions, depression of consciousness, coma, blockade of the vasomotor center, although its toxicity is also considered low. The minimum toxic dose of lidocaine is 6.4 mg/kg body weight.
Low risks and their complete absence are different concepts, so it would also be appropriate to determine the dosage of the anesthetic at which a side effect may develop, and remember the list of adverse reactions .
- Local undesirable side reactions are swelling, inflammation at the injection site due to the vasodilator effect.
- Local anesthetics are toxic to the nerve when applied in too large doses.
- Allergic reactions are typical for local anesthetics with an ester structure. Cross-reactions are possible between them, since the same metabolites are formed during hydrolysis - PABA (para-aminobenzoic acid).
Resorptive (additional) side effects are determined by the degree of drug toxicity and dose, and are manifested in excitable tissues and organs (central nervous system, myocardium, autonomic ganglia):
- hypotension;
- dizziness;
- nausea;
- tachycardia;
- excessive stimulation of the central nervous system, and then depression;
- convulsions;
- respiratory arrest;
- coma.
Lidocaine is quickly distributed into tissues. First it enters tissues with a high rate of blood supply (heart, brain, kidneys, lungs, liver, spleen), then into adipose and muscle tissue. Easily penetrates histohematic barriers, including blood-brain and placental. Metabolized in the liver with the participation of microsomal enzymes with the formation of metabolites: monoethylglycine exilidide and glycine exilidide. The half-life of metabolites is 2 and 10 hours, respectively. If liver function is impaired, the half-life may increase.
The data presented allow us to summarize that the optimal drug in terms of anesthetic effect, duration of action and low risk of unwanted side reactions is lidocaine.
Lidocaine in contouring preparations
Let's look at a classic example. The average patient weighing 60–70 kg comes to see a cosmetologist. If such a patient has a deficiency of integumentary tissue and there is a direct indication for facial contouring, the primary area of correction is the middle third of the face. On average, 3 ml of fillers are consumed on the zygomatic region and infraorbital grooves, which differ in rheological properties, but contain a standard dosage of lidocaine equal to 0.3% per 1 ml. Therefore, in order to obtain a certain risk of side effects, it is necessary for a patient with the specified body weight to inject about 128 ml of filler with lidocaine in one procedure. It is simply impossible to inject such a volume into facial tissue as part of a one-step correction.
This is confirmed by the fact that for over 10 years, all the largest listed filler production companies in the world have been using lidocaine lines that have a European CE certificate, a registration certificate in the Russian Federation and an FDA certificate, allowing the free import and use of drugs in medical practice in the United States.
Returning to the use of drugs in which the manufacturer has previously included an anesthetic, it is worth noting:
- the presence in its composition exclusively of lidocaine and always in a safe concentration;
- international experience of use over 10 years.
Not all companies represented on the Russian and world stage have fillers with a lidocaine component. This is due to the high cost of registration and the duration of clinical trials in the EU. That is, the problem of the existence of a small number of brands of fillers with lidocaine lies not in the fears of the company, but in the resources spent.
The Teoxane laboratory, which has a global history and a total experience in producing products based on reticulated and native hyaluronic acid for over 15 years, is one of the market leaders and provides a unique clinical research base, as well as three sub-lines of fillers, two of which contain 0.3% lidocaine in its composition (see table).
Table. Teosyal® line of dermal fillers - expert set (open the picture in a new tab to view in large size)
The presence of lidocaine in the filler is especially important when it comes to correcting areas of psychological problems (periorbital), with a high density of pain receptors (perioral) or introducing drugs with a high viscosity index (for example, Ultra Deep on the periosteum).
Another nuance in the use of fillers with lidocaine lies in the speed of administration. Having a pH of 7.8, when administered rapidly it can cause pain due to its higher pH compared to the pH of the extracellular fluid (7.2–7.4). Therefore, any extrusion, especially of viscous fillers, must be carried out slowly and evenly [3].
Remembering that same initial patient, suffering from a number of phobias, we can safely say that the procedure using Teosyal® fillers will be painless, quick and revealing for him and will serve as a good start in building a long-term relationship with the doctor. After such a patient “tests” the procedure and finds it painless, all subsequent visits will not be accompanied by any phobias.
The article was published in the journal “Injection methods in cosmetology” No. 3/2020
As an advertisement
Literature
- Story GW, Vlaev I., Seymour B., et al. Dread and the disvalue of future pain. PLoS Comput Biol 2013; 9(11): e1003335.
- Derry S, Wiffen PJ, Moore RA, et al. Topical lidocaine for neuropathic pain in adults. Cochrane Database Syst Rev 2014; 2014(7): CD010958.
- Cepeda MS, Tzortzopoulou A, Thackrey M, et al. Adjusting the pH of lidocaine for reducing pain on injection. Cochrane Database Syst Rev 2010; (5):CD006581.
Ceftriaxone during pregnancy and breastfeeding
The drug is contraindicated in the first trimester of pregnancy. If it is necessary to prescribe to a nursing woman, the child should be switched to formula.
Reviews of Ceftriaxone during pregnancy confirm that the drug is indeed a very powerful and very effective antibacterial agent that can not only cure the underlying disease, but also prevent the development of its complications.
Considering that the drug (like other antibiotics) has side effects, it is prescribed only in cases where potential complications of the disease could be more harmful than the use of the drug (in particular, for infections of the urogenital tract, to which pregnant women are very susceptible).
Why is the antibiotic dissolved with the anesthetic Procaine?

Real Ceftriaxone is sold only in powder form. But this antibiotic is intended for intramuscular or intravenous administration. Injections require liquid solutions. Ceftriaxone can be diluted with either distilled water or anesthetics.
Ceftriaxone can be diluted with distilled water. But in this case, when administered intravenously or intramuscularly, the patient experiences severe pain. Therefore, the anesthetic Novocaine or Lidocaine is used as a solvent. The latter is more preferable because it is less allergic.
The doctor chooses which analgesic to use as a solvent, but it depends on:
- From the place where the doctor recommended injecting the medicine.
- From the tolerance of one of the anesthetics. Therefore, before prescribing injections, a test is made to determine the tolerance of the anesthetic substance.
Is it possible to dilute Ceftriaxone with Novocaine? It can be diluted if there are no contraindications to the use of an analgesic. Recommendations for the use of the solvent are given by the attending physician. You need to understand that both remedies can provoke severe allergies.
Initially, you need to study the instructions, then you can start preparing the medicine. The diluted medicine should be used only in the amount recommended by the doctor.
Reviews of Ceftriaxone
Ceftriaxone is a potent antibiotic (reviews from doctors confirm this fact), which helps cure the disease in a short time and with a minimum number of side effects. It is allowed to be used for children and during pregnancy (exception - 1st trimester).
According to the patients themselves, the main disadvantage of the drug is that the injections are very painful.
In reviews of Ceftriaxone injections for children, to facilitate the procedure, mothers (on the advice of the attending physician) are recommended to use Emla , which is a local anesthetic. It is applied in about half an hour to the intended injection site.
Is the lidocaine solution better?
It is believed that it is better to dilute the powder preparation with Lidocaine.
Procaine may:
- Provoke the appearance of anaphylactic shock.
- Reduces the bactericidal effects of the drug.
The instructions for use recommend using a 1% analgesic composition. You just need to say that the pharmacy does not always have a 1% solution, more often there is 2%.
Therefore, doctors recommend:
- Dilute 2% analgesic with distilled water to obtain 1%. To do this, draw 1 ml of Lidocaine into the syringe, and then 1 ml of water.
- Introduce the resulting liquid into a bottle with powder. Shake the mixture well. The liquid should sit for a minute or two. Then it is ready for use.
- The resulting liquid is used for intramuscular injections. Usually the injection is given in the upper quadrant of the gluteal muscle. The procedure must be carried out leisurely, slowly, so as not to provoke additional pain.
Why is it better to dilute Ceftriaxone with Lidocaine? Patients note that such mixtures are less painful. Not freshly prepared medicine can increase pain.
However! Lidocaine antibiotic is used for intramuscular administration only. For intravenous administration, use a solution of Ceftriaxone with Novocaine or distilled water.
For adults, the instructions for use recommend injections 2 times a day. An adult patient receives 0.5 g at a time. If the disease is severe, the dose can be increased to 2 - 4 grams per day.
Ceftriaxone price, where to buy
How much does an antibiotic cost in Russian pharmacies? The price of Ceftriaxone injections varies depending on which company produces it, as well as the number of ampoules in each package and the concentration of the active substance in the vial.
The price of Ceftriaxone in Russian pharmacies is from 30 rubles per bottle.
The price of Ceftriaxone in Ukraine is from 15 UAH. per bottle of 1 g. At the same time, there is no significant difference between prices in the capital's pharmacies and pharmacies in other cities (Kharkov, Dnepropetrovsk, Lvov).
It is impossible to buy Ceftriaxone tablets. The drug is intended exclusively for parenteral administration.
- Online pharmacies in RussiaRussia
- Online pharmacies in UkraineUkraine
- Online pharmacies in KazakhstanKazakhstan
ZdravCity
- Ceftriaxone powder for injection solution for IV and IM injection.
1g bottle of Rapharma JSC 45 rub. order - Ceftriaxone powder prig solution for intravenous and intramuscular injection. fl. 1gPAO Biosintez
43 RUR order
- Ceftriaxone por. ready solutions for intravenous and intramuscular injection. 1g 10pcs Borisov Medical Preparations Plant OJSC
RUR 797 order
- Ceftriaxone powder for injection solution 1g bottle JSC Pharmaceutical company LEKKO
47 RUR order
- Ceftriaxone-AKOS powder for the preparation of a solution for intravenous and intramuscular administration 1 g 1 pc per individual. upSintez OJSC
45 rub. order
Pharmacy Dialogue
- Ceftriaxone (vial 1g i.m., i.v.) Biosynthesis OJSC
38 rub. order
- Ceftriaxone (vial 1g i.v. i.m. individual pack)DECO Company
45 rub. order
- Ceftriaxone (vial 1g IM, IV) Biosynthesis OJSC
51 RUR order
- Ceftriaxone (vial 1g IM, IV)Biokhimik JSC
77 RUR order
- Ceftriaxone (portion d/d-ra i/v, i/m fl 1g No. 1 + solution water amp 5 ml No. 2) Biokhimik JSC
RUB 187 order
show more
Pharmacy24
- Ceftriaxone 1 g N10 powder PAT "Kievmedpreparat", Ukraine
151 UAH.order - Ceftriaxone-BHFZ 500 mg No. 1 powder PAT NVC "Borshchagivsky chemical-pharmaceutical plant", Kiev, Ukraine
11 UAH order
- Ceftriaxone-Darnitsa 0.5 g N5 lyophilisate for the preparation of solution for injection PrAT" Pharmaceutical company "Darnitsa", Ukraine
58 UAH order
- Ceftriaxone-Darnitsa 1 g No. 5 solution PrAT” Pharmaceutical company “Darnitsa”, Ukraine
72 UAH order
- Ceftriaxone 1.0 g No. 1 powder AT Lekhim-Kharkiv, Ukraine
13 UAH order
PaniPharmacy
- Ceftriaxone bottle Ceftriaxone sodium salt powder for injection 1g Ukraine, Kievmedpreparat OJSC
169 UAH order
- CEFTRIAXONE bottle Ceftriaxone powder for injection 1g No. 5 Ukraine, Lekhim-Kharkov JSC
74 UAH order
- Ceftriaxone bottle Ceftriaxone sodium salt powder for injection 0.5g Ukraine, Kievmedpreparat OJSC
110 UAH order
- Ceftriaxone bottle Ceftriaxone powder for injection 1g bottles No. 40 Ukraine, Darnitsa ChAO
681 UAH order
- CEFTRIAXONE bottle Ceftriaxone powder for injection 1g Ukraine, Lekhim-Kharkov JSC
15 UAH order
show more
Procedure for preparing the solution
- Collect everything you need and place it on a pre-prepared and thoroughly disinfected wide plate or dish.
- Wash your hands thoroughly. For this, laundry soap with the highest alkalinity is best suited. Wipe with a clean towel and disinfect with an antiseptic solution. If there are no sterile medical gloves, then special attention should be paid to hand cleanliness.
- Using tweezers or other available means, remove the protective valve from the lid of the bottle with powder.

- Both the rubber cap and the ampoule at the site of the break must be thoroughly disinfected.
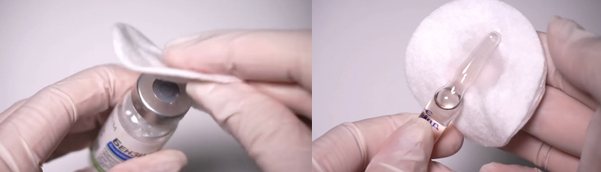
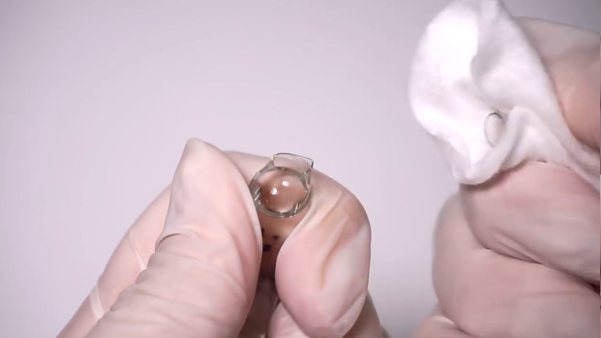
- Open the ampoule with the special file included with the package. If such a tool is not included, you simply need to break off the upper part of the ampoule by attaching a piece of cotton wool or a sterile swab to it.
- Replace the needle on the syringe with the one with which the solution will be mixed. As a rule, for this purpose a needle of a larger diameter is used than the one with which the injection is supposed to be given. Now we draw the solvent from the ampoule into the syringe.

- We pierce the rubber cap of the medicine bottle and, pressing on the piston, introduce all the solvent there.

Then, without removing the needle and syringe, you need to carefully shake the bottle until the powder dissolves. You can find out what the finished solution should look like in the instructions for the drug.Attention
To avoid compromising sterility, never touch the needle with your hands during manipulations to prepare the solution.
- The solution is ready. Now we remove the syringe from the bottle and change the needle to the one that we will use for the injection. Already with this needle, we draw the solution from the bottle, turning it upside down so that the tip of the needle is immersed in the liquid.

- After you have filled the entire solution into the syringe, carefully remove the needle from the bottle. Turn the syringe over with the piston down and lightly tap your fingers to shake the solution so that all the air bubbles collect at the top. Then, by pressing the plunger, remove air from the syringe. Droplets of solution that appear usually indicate that there is no more air in the syringe.
- We put a cap on the needle (if you are not going to inject immediately). Solution in a syringe. Everything is ready for the procedure.
We recommend reading:
- How to place an IV?
- Installation of an intravenous catheter and rules for caring for it
- How to give a subcutaneous injection to yourself?
- How to make an intradermal injection yourself?
- Blood clotting mechanism (INR). Measurement and norms
- How to give yourself an intramuscular injection?
- How to choose a needle and syringe for giving an injection
Partners recommend:
***