Immunoglobulin when planning pregnancy
home
Articles
Immunoglobulin when planning pregnancy
Immunoglobulin is an immunostimulating agent that helps the body fight viruses and bacteria. Reduces the risk of infection in immunocompromised individuals. The lack of immunity can be chronic or caused by certain situations. This number also includes pregnancy. A woman’s body reduces the level of immunity so that the fetus is not rejected by it as a foreign body. Therefore, immunoglobulin can be a very important link in planning pregnancy. Prescribed mainly for problems with pregnancy.
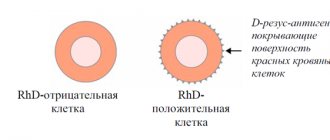
There are two types of immunoglobulin: “normal human” and “anti-D immunoglobulin”. The second is used when there is a conflict between the Rh factors of the blood of the mother and fetus. The first is prescribed if there are serious indications or a woman’s immunodeficiency during pregnancy or during planning. The instructions for the drug say that its effect on pregnancy is not fully known.
Immunoglobulin is administered in drops; the dosage and frequency of use are prescribed by the doctor, based on the individual characteristics of the woman’s body, the course of pregnancy, and the duration. It is important to remember here that improper use of immunoglobulin during planning and pregnancy can have a negative effect.
As stated in the article, there are serious concerns about taking this drug. Such as the threat of miscarriage (and at any stage), interruption of an ectopic pregnancy, abortion, abdominal injuries and some others. If, when planning a pregnancy, an immunodeficiency is diagnosed in the mother, in this case, the doctor may decide to prescribe the drug, since it compensates for the deficiency of IgG.
Side effects usually do not last long. Their list includes joint pain, shortness of breath, itching, dry cough, fatigue, fever, nausea, tachycardia and others.
The topic of immunoglobulin is vast and the justification for its use depends on many factors. Unfortunately, it is impossible to make the right decision after reading the article. We recommend that you contact a gynecologist who, based on an analysis of your situation, will select an individual treatment strategy for you. DNA Clinic provides pregnancy planning and management services. With us, you will undergo medical procedures, on the basis of which our gynecologist will create a treatment or prevention program for you. You can make an appointment here.
Return to list
IMMUNOGLOBULIN ANTI-RHESUS HYPERROW S/D
Directions for use and doses
Before administration, ampoules with the drug are kept for 2 hours at room temperature (+20±2)°C.
To avoid foam formation, the drug is drawn into a syringe with a wide bore needle. The drug cannot be stored in an opened bottle. Cannot be administered intravenously. Human anti-rhesus immunoglobulin Rho(D) is administered in one dose (1500 IU), sometimes two doses (3000 IU), intramuscularly once: to a postpartum woman - within 72 hours after birth, in case of termination of pregnancy - immediately after the end of the operation. The following criteria must be met:
1. The mother must be Rh negative and must not already be sensitized to the Rho(D) factor.
2. Her child must be Rh positive.
If the drug is given before delivery, it is essential that the mother receives another dose of the drug after the birth of her Rh-positive baby within 72 hours of delivery. If it is determined that the father is Rh negative, there is no need to administer the drug.
Pregnancy and other conditions associated with pregnancy and childbirth
1. For prophylaxis during the postpartum period, one dose (1500 IU) of HyperROU® S/D should be administered, preferably within 72 hours after birth. The need for a certain dose in the case of a full term pregnancy varies depending on the volume of fetal blood entering the mother's bloodstream. One dose (1500 IU) contains a sufficient amount of antibodies to prevent sensitization to the Rh factor, if the volume of fetal red blood cells entering the mother's bloodstream does not exceed 15 ml. In cases where a larger volume of fetal red blood cells (more than 30 ml of whole blood or more than 15 ml of red blood cells) is expected to enter the maternal circulation, fetal red blood cells should be counted using an approved laboratory technique (for example, the modified Kleihauer and Vetka acid washout-stain method ) to establish the required dosage of immunoglobulin. The calculated volume of fetal red blood cells entering the mother's bloodstream is divided by 15 ml and the number of doses of HyperROU® S/D that must be administered is obtained. If the presence of more than 15 ml of fetal red blood cells is expected, or the dose calculation results in a fraction, round the number of doses up to the next whole number (for example, if the result is 1.4, administer 2 doses (3000 IU) of the drug).
2. For prophylaxis during the prenatal period, one dose of the drug (1500 IU) should be administered at approximately the 28th week of pregnancy. This must be followed by another dose (1500 IU), preferably within 72 hours after birth, if the newborn baby is Rh positive.
3. If pregnancy continues after the threat of abortion arises, at any stage of pregnancy it is recommended to administer one dose (1500 IU) of the drug. If it is suspected that more than 15 ml of fetal red blood cells have entered the maternal bloodstream, the dose must be adjusted as described in point 1 above.
4. After spontaneous abortion, induced abortion or termination of ectopic pregnancy during pregnancy more than 13 weeks, it is recommended to administer one dose (1500 IU) of the drug. If it is suspected that more than 15 ml of fetal red blood cells have entered the maternal bloodstream, the dose must be adjusted as described in point 1. If the pregnancy is terminated at less than 13 weeks, a single mini-dose of HyperROU® S/D (approximately 250 IU) may be used.
5. After amniocentesis, either at 15-18 weeks of pregnancy, or during the third trimester of pregnancy, or if abdominal trauma occurs during the second and/or third trimester, it is recommended to administer one dose (1500 IU) of the drug. If it is suspected that more than 15 ml of red blood cells have entered the mother's bloodstream, the dose must be adjusted as described in point 1. If abdominal trauma, amniocentesis or other adverse circumstance requires administration of the drug at 13-18 weeks of pregnancy, another dose should be administered (1500 ME) at 26-28 weeks. To maintain protection throughout pregnancy, the concentration of passively obtained antibodies to Rh0(D) should not fall below the level necessary to prevent an immune response to Rh-positive red blood cells. The half-life of human anti-rhesus immunoglobulin Rho(D) is 23-26 days. In any case, the dose of the drug should be administered within 72 hours after birth if the baby is Rh positive. If delivery occurs within 3 weeks of the last dose, the postpartum dose can be discontinued (unless more than 15 ml of fetal red blood cells have entered the maternal circulation).
Allergies and pregnancy: myths and reality
For many women, pregnancy is not only a long-awaited joy, but also a cause for concern. The information space is replete with articles about a variety of risk factors. Some of which really require attention, while others are nothing more than a myth.
The “danger” of allergies in a pregnant woman for the health of the fetus is one of the common causes of concern. How much concern is justified? Let's figure it out.
Myth No. 1: exacerbation of allergies during pregnancy - the risk of “allergization” of the child
The mechanism for the development of an allergic reaction is identical to that for any inflammation. Foreign object – production of antibodies – binding, removal and destruction of antigen – recovery.
In the case of allergies, class E antibodies serve as such “protection”, and some elements of the environment or food serve as a foreign object. Produced by the body after the first encounter with an “unpleasant” object, IgE is stored in the blood as “memory” cells and instantly initiates an “attack” (the release of histamine and similar substances) upon repeated encounter with the allergen.
However, due to their large size, class E antibodies are not able to penetrate the placental barrier, and the point of application of histamine and similar substances is only the “target” tissues of the allergic person (skin, respiratory tract and conjunctiva). Thus, neither IgE nor the “products” of its activity are capable of having any serious effect on the fetus.
Myth No. 2: Pregnancy causes an exacerbation of allergies.
Pregnancy is known for some “muffled” immune processes. Without a relative decrease in protective forces, the fetus would be rejected as a foreign object, but thanks to adrenal hormones this does not happen.
Normally, cortisol levels in a pregnant woman remain elevated until delivery. This weakens the reactivity of her immune system, not only against microorganisms, but also allergens, allowing her to “rest” from unpleasant allergy symptoms.
However, in approximately 10-30% of expectant mothers, allergies still make themselves felt. This may be due to a number of reasons, including genetic characteristics of the immune and hormonal status.
Myth No. 3: A blood test can predict possible allergies.
A general immunoglobulin E blood test serves to confirm the allergenic nature of existing symptoms and cannot be a risk marker.
Skin allergy tests can help predict the development of an allergic reaction in advance. The study involves applying allergens to a previously “scratched” area of skin with further assessment of the reaction. True, skin tests are not recommended during pregnancy, and the tests themselves can be false negative, due to the “work” of cortisol. While testing blood for class E antibodies to a specific allergen has no contraindications, and the high sensitivity of the test allows you to detect even the most minor changes. The level of immunoglobulin E to the allergen shows the level of “sensitization” - the body’s possible sensitivity to the allergen.
It must be said that to confirm the diagnosis, in combination with IgE, a general blood test with leukocyte count (focus on eosinophils) and eosinophil cationic protein (for hay fever) are indicated.
Obtaining increased values in the results is a justification for further examination, aimed either at searching directly for an individual allergen, or identifying a reaction to a specific group.
It is worth noting that the presence of an allergy comes as a “surprise” for some, since in a mild form the symptoms may be no different from skin diseases, acute respiratory viral infections, and even food intolerance. And due to the complex structure of some allergens, hypersensitivity, for example, to birch, manifests itself in a reaction when eating peaches.
Thus, an allergy as such is not capable of harming the fetus, normally should not appear during pregnancy, it is not possible to predict its occurrence, and a simple and effective blood test can help determine the existing reactivity.
Normal human immunoglobulin - solution for infusion
special instructions
The drug is intended for single use.
After opening the bottle, the consumer is responsible for the duration of storage and storage conditions. Partially used drug cannot be stored or used. Unused drug and consumables should be disposed of in an appropriate manner.
The drug should not be used after the expiration date.
Patients should be closely monitored and monitored for any symptoms during the infusion period.
Persons who are injected with the drug must be under medical supervision for 30 minutes after its administration.
Infusion sites should be provided with anti-shock therapy.
The patient's condition should be closely monitored during drug infusion.
Some adverse reactions may occur more frequently:
- in case of high rate of administration; - in patients with hypogammaglobulinemia or agammaglobulinemia with or without IgA deficiency; - in patients who receive normal human immunoglobulin therapy for the first time, or in rare cases, when switching to another immunoglobulin drug, or after a long break after the previous infusion.
Possible complications can be avoided by making sure that:
- the patient does not exhibit hypersensitivity to normal human immunoglobulin with slow administration of the drug (0.5 mg/kg body weight/min); - During and after the infusion period, all symptoms experienced by patients are carefully monitored. In particular, patients who have not previously received human normal immunoglobulin therapy, who are switching from treatment with another intravenous immunoglobulin product, or who have had a long interval since the previous infusion, should be monitored during the first infusion and for the first hour after the first infusion to identify potential adverse events. All other patients should be observed for at least 30 minutes after administration of the drug.
If an adverse event occurs, the rate of administration should be reduced or the drug should be discontinued. The treatment required depends on the nature and severity of the adverse event.
If shock develops, standard treatment for shock conditions should be used.
All patients require adequate hydration before starting intravenous human immunoglobulin.
Hypersensitivity True hypersensitivity reactions are rare. They can occur in very rare cases with IgA deficiency with anti-IgA antibodies. Rarely, normal human immunoglobulin may cause a decrease in blood pressure with the development of an anaphylactoid reaction, even in patients who previously tolerated normal human immunoglobulin therapy well.
Hemolytic anemia Intravenous human immunoglobulin preparations may contain antibodies against blood group antigens, which can act as hemolysins and bind in vivo to red blood cells, which can cause a positive direct antiglobulin test (Coombs test) and, rarely, hemolysis. Hemolytic anemia may develop after therapy with intravenous human immunoglobulin preparations as a result of increased sequestration of red blood cells. Isolated cases of renal dysfunction and/or renal failure or disseminated intravascular coagulation syndrome associated with hemolysis have been reported.
The development of hemolysis is associated with the following risk factors:
high doses, whether administered as a single dose or in separate doses over several days; as well as blood groups A (II), B (III) and AB (IV) in combination with the concomitant presence of an inflammatory process. When treating patients with blood groups A (II), B (III) or AB (IV) with high doses of the drug for indications other than PID, extreme caution is recommended.
There are isolated reports of hemolysis in patients with PID receiving replacement therapy. Monitor clinical signs and symptoms of hemolysis in patients receiving intravenous human immunoglobulin therapy. If signs and/or symptoms of hemolysis occur during or after intravenous immunoglobulin infusions, the prescriber should consider discontinuing further treatment.
Aseptic meningitis syndrome (ASM) Cases of aseptic meningitis syndrome have been reported during treatment with intravenous immunoglobulin preparations. After discontinuation of intravenous immunoglobulin, MAS remission occurred within several days without any consequences. This syndrome usually begins within a few hours to 2 days after treatment with intravenous immunoglobulin. When analyzing cerebrospinal fluid, pleocytosis of up to several thousand cells per mm3 is often observed, usually due to cells of the granulocyte lineage, as well as an increased protein concentration, up to several hundred mg/dl. MAS may develop more frequently with the use of intravenous immunoglobulin in high doses (2 g/kg).
Thromboembolic complications There is clinical evidence of an association between the use of intravenous human immunoglobulin and the occurrence of thromboembolic complications, such as myocardial infarction, acute cerebrovascular accident (including stroke), pulmonary thromboembolism and deep vein thrombosis, which are presumably associated with a relative increase in viscosity blood with the introduction of a large amount of immunoglobulins. Caution must be exercised when prescribing and administering intravenous immunoglobulin infusions to obese patients and patients with previously established risk factors for thrombotic complications, such as advanced age, hypertension, diabetes mellitus, thromboembolism or a history of cardiovascular disease, hereditary or acquired thrombophilia, prolonged periods of impaired mobility, patients with severe hypovolemia and patients with diseases in which there is an increase in blood viscosity.
Acute renal failure Cases of acute renal failure have been identified in patients receiving intravenous human immunoglobulin therapy. In most cases, risk factors were identified, such as pre-existing renal failure, diabetes mellitus, hypovolemia, excess weight, concomitant treatment with nephrotoxic drugs, or age over 65 years. If renal failure develops, therapy with intravenous human immunoglobulin should be interrupted. It should be noted that among the reports of cases of renal dysfunction or renal failure developing while taking registered human immunoglobulin preparations, the proportion of preparations containing sucrose as a stabilizer was disproportionately high. Thus, for patients who are at risk, the use of intravenous immunoglobulin preparations that do not contain sucrose is recommended.
In patients at risk of developing acute renal failure or thromboembolic complications, intravenous immunoglobulin preparations should be administered at the minimum infusion rate and dose possible.
Effect on diagnostic tests After administration of immunoglobulins, the number of various passively transferred antibodies temporarily increases in the patient's blood, which can lead to a false-positive result in serological tests.
Passive transfer of antibodies to red blood cell antigens, such as A, B, and D, may cause an incorrect result in some serological tests for red blood cell antibodies (eg, Coombs test), reticulocyte count test, and haptoglobin test. Due to the presence of dextrose in the drug, it is possible to increase the concentration of glucose in the patient’s blood, which affects the result of its determination. Elevated blood glucose concentrations are determined during the period of drug administration and within 15 hours after drug administration. This fact must be taken into account when prescribing therapy for patients with diabetes.
Safety information regarding infectious agents The drug is produced from human plasma. Standard measures to prevent the transmission of infections resulting from the use of medicinal products made from human blood or plasma include selecting donors, screening individual donations and plasma pools for specific markers of infection, and incorporating effective manufacturing steps to inactivate and/or remove viruses . Despite this, when using drugs made from human blood or plasma, the possibility of transmission of infectious agents cannot be completely excluded. This provision also applies to unknown or new viruses and other infectious agents. Measures taken to ensure antiviral safety are considered effective for enveloped viruses such as HIV, hepatitis B and C viruses, and for non-enveloped viruses such as hepatitis A virus and parvovirus B19. There is encouraging clinical experience indicating that there is no transmission of hepatitis A virus and parvovirus B19 with human immunoglobulin preparations, and it is also suggested that the presence of antibodies makes a significant contribution to viral safety. It is recommended that each time a drug is used, the name and lot number of the drug administered to the patient is recorded to maintain a link between the patient and the drug lot. You should also record the date of release, expiration date, name of the manufacturer, date of administration and adverse reactions to the drug.
Impact on the ability to drive vehicles and machinery. Some adverse reactions associated with the action of the drug may affect the ability to drive a vehicle or operate machinery. For patients who have experienced adverse reactions during the administration of the drug, driving a vehicle or moving machinery is possible only after the symptoms of adverse reactions disappear.