What is testosterone propionate?
Testosterone propionate is a “short-lived”, synthetic, that is, chemically synthesized, anabolic androgenic steroid.
It ranks second in demand among athletes taking anabolic steroids.
Slang name: “Propik”, “Prop”, propionate
It is worth noting that Testosterone Propionate is the first testosterone that was synthesized and commercially released for medical use from 1937 to 1960.
In bodybuilding, testosterone propionate, due to its characteristics, is used mainly during the “cutting” period, but is excellent for building muscle mass and strength, with some reservations, which will be discussed below.
Observing the statistics of search queries, I very often find the request “buy testosterone propionate tablets”
I will probably disappoint someone, but testosterone propionate is only available in injections. Propionate, like any other testosterone, (except methyltestosterone) does not exist in tablets. And you should give up fruitless attempts to find one.
Side effects of injections
When using testosterone injections, men may experience side effects:
- acne, itchy skin;
- dizziness;
- weight gain;
- urinary disturbance;
- early puberty in adolescents;
- impaired spermatogenesis, erection, priapism (prolonged persistent erection accompanied by pain);
- atrophy of the testicles, seminiferous tubules;
- high blood pressure, myocardial infarction;
- sleep disturbance;
- gastrointestinal bleeding;
- increased sweating.
How and how much to inject testosterone propionate?
The period of maximum effective action of propionate is one day, which suggests that you should inject propionate at least every other day. Ideally, you should inject propic every day, which, at least psychologically, is not convenient. After all, not everyone is ready to “punch” their ass every day.
And what's the point? For mass gain, it is much easier to use any of the “long-lasting” testosterone esters.
Propionate is injected mainly into the large muscles of the body - the gluteal, thigh muscles. Less commonly, testosterone propionate is injected into the deltas.
By the way, few people know that propionate can be administered subcutaneously, i.e. into the fat layer on the abdomen. An insulin syringe is used for this.
The recommended basic dosage for beginners is 50 mg, every other day or every day. Experienced athletes use 100 mg. every day and above.
I do not consider the use of propionate to gain muscle mass justified, since testosterone ethantate is best suited for these purposes.
But for “drying”, advanced and competitive athletes, propionate is best suited.
Also, testosterone propionate “must feb” is a “exit” from the course where “long” steroid esters are used.
In such cases, propionate begins to be placed 2-3 weeks before the long ether is expected to “complete its work.”
The use of testosterone propionate in this way allows you to accurately understand when you need to start PCT, because propionate will be completely eliminated from the body a maximum of 4-6 days after the last injection, and with “long” esters the period of complete elimination is difficult to calculate, because it “floats” from 3 weeks or more.
To accurately understand when to start PCT, you need to get tested for total testosterone. The analysis is carried out when you have approximately calculated that the ether has already completed its work in the body.
We described what values of your own test you should focus on in the article “How to conduct PCT correctly”
Starting PCT when the dough you injected is still active in the body does not make sense and will not bring any benefit, since restoration of the hypothalamus-pituitary-testes arc will not take place in this case.
As a result, PCT will be, at a minimum, incomplete.
You won't recover. That is, you will not reach normal levels of your own testosterone, which will subsequently lead to a “collapse” of muscle mass and strength.
In addition, the use of propionate at the “exit” of the cycle will allow us, for several more weeks after the ester, to maintain high working concentrations of testosterone in the blood, and in fact finish the course with a better result than we would have simply canceled the long ester and waited until it “ will fizzle out."
Testosterone in men and infertility
Here's what testosterone levels affect in men:
- responsible for the formation of male-type genital organs;
- promotes muscle growth;
- improves heart condition;
- increases calcium deposition in bones;
- responsible for the structure of the larynx and the entire body according to the male type;
- is the main cause of specific male behavior and mental reactions;
- forms the appearance of hair and adipose tissue strictly in certain places;
- promote sperm production.
Both low and high testosterone levels can be to blame for infertility. In the second case, testosterone suppresses the production of LH, which increases the production of follicle-stimulating hormone. This inhibits sperm division.
How long is testosterone propionate excreted and effective?
“Propik” begins to act in the body almost immediately after the injection. Maximum activity is achieved within the first 24 hours after an injection of testosterone propionate, followed by a decline within two to three days.
Thus, the half-life of this steroid is 1-2 days.
In fact, if we talk about the elimination of the drug, in terms of the time when you need to start PCT, then PCT after propionate can and should be started after about three half-lives - about 6 days after the last injection.
If we mean doping - monitoring for the presence of propionate metabolites in the blood, then detection of such metabolites is possible within a period of 40 to 60 days.
So, if you expect that you will need to undergo doping control, you should stop using propionate two months before the expected test.
Very often, people ask if taking propionate will affect my CBC, can doctors detect that I'm taking steroids?
Answer - No, they cannot.
A complete blood test cannot show that you are using any steroid drugs.
How much testosterone propionate can you gain?
As mentioned above, using propic for mass gain is not rational.
During the drying process, we work to reduce the percentage of body fat using a caloric deficit in the diet. Therefore, during the drying process, weight gain is in principle impossible.
But if you still love “sado-maso”))) and decide to use propik to gain muscle mass, then you should know and understand that no one can accurately predict how much you will gain.
Everyone is different. They have different genetics, metabolism, etc. In addition, the key factor in gaining weight during the cycle is nutrition.
You can “pour” testosterone into yourself in grams, but you won’t gain it unless you create a calorie surplus.
Therefore, if someone confidently tells you some numbers, you should know that this is an amateur who does not understand anything about this issue.
Which brand of testosterone propionate is better?
A very common question is: Which brand of propionate is best to buy?
I will speak for our store - Pharma UA.
Specifically, in terms of quality, I cannot single out any company. And that's why:
Over our long history of working in the sports pharmacology market, we have only sold products from those manufacturers that we have used and use ourselves, and we can guarantee the quality and originality of these drugs.
In addition, both we and our clients were tested more than once or twice after injections of propionate from different manufacturers. Analyzes showed the reference amount of testosterone in the blood after injections.
Of course, there are always people who prefer to buy one company or another. But this is more a matter of personal preference, recommendations from friends, etc., than an objective choice of a drug based on its quality characteristics.
If we look at the sales ranking, we will put testosterone propionate Balkan (Propandrol) in first place, second place belongs to EPF. The demand for other manufacturers is approximately the same.
In fact, the difference in testosterone propionate from different manufacturers lies in the use of different types of oil in which the active substance of the propionate steroid is dissolved. The concentration of the active substance is the same in all cases - 100 mg per 1 ml. Excluding the obvious underground. In “under” products, the amount of active ingredient can vary greatly, usually to a lesser extent. Therefore, I advise you to avoid buying testosterone propionate from “know-name” companies.
You can buy propionate from any manufacturer from us and we guarantee that it will work and the amount of active ingredients in it corresponds to the declared amount.
What level of testosterone should a man have?
What is increased testosterone in men?
These figures are above 33 nmol/l in representatives of the stronger sex 18-50 years old, and above 20 nmol/l in those over the age of 50.
The norm of free testosterone in men 18-50 years old is 5.5-42 picograms in 1 ml of blood (or 5.76-33 nmol/l). After 50 years, the hormone level decreases to 5.4-19.5 nmol/l.
Signs of increased testosterone in men will not be noticeable externally if the hormone level is 20-30% higher. If the hormone concentration is significantly higher, the following are noted:
- baldness;
- excessive hair growth on the chest, legs, back, face;
- frequent headaches;
- insomnia;
- aggressive behavior;
- growth of muscle mass.

Why is testosterone propionate harmful?
The question is most likely about the side effects of propionate, which we will discuss below.
You must understand that any medical drug has side effects, and it is easier to count on your fingers those drugs that do not have shelves. (I don't even know them)
And when it comes to steroids and the side effects of their use, then real hysteria and “trash” begins.
Very often, even qualified doctors who have not delved into the topic of AS are captive of public stereotypes about the “terrible harm” of steroids.
And what heartbreaking stories about the side effects of AS can be found on the Internet...
Someone’s “liver fell off”, “the kidneys stopped working”...
I will say this, all the horror stories that you may have heard about the dangers of steroids are a complete exaggeration.
For example, regular aspirin will give a huge head start to propionate and other AS in terms of side effects. But we easily take aspirin, without thinking about its potential harm, because it is a common drug for us.
But you should know that, according to statistics, in the United States, which is the world’s largest audience of steroid users, aspirin and various types of painkillers occupy almost the first places for the reasons for people visiting and hospitalizing people with symptoms of an overdose of these drugs. Many of these cases are fatal.
Whereas requests for help from an overdose of AS occur in isolated cases. And they only concern the side effects that have arisen. Not a single case of death from an overdose of AS has been recorded in the world.
In principle, an “overdose” of ACC, a word that I would not like to use when describing AS, since an “overdose” of a “propic” only entails a greater frequency and the likelihood of “catch” one or another “side effect”. Toxic damage to the body does not occur in the event of an “overdose”.
Based on what was written above, it becomes clear that the problem of the harm of testosterone propionate and steroids in general is greatly exaggerated and does not correspond to reality.
I'm not trying to say that testosterone propionate doesn't have side effects, it does. But in the vast majority of cases, using propionate in recommended dosages, you won’t even notice them.
But if side effects do occur, almost all of them are reversible and can be controlled with the use of appropriate medications. The exception is advanced cases of gynecomastia, when cosmetic surgery to remove it is necessary.
Possible side effects from the use of testosterone propionate
- aromatization - the conversion of testosterone under the action of the aroma enzyme into estradiol and the possible subsequent development of estrogen-related side effects - gynicomast, water accumulation, fat deposition.
Aromatization is easily removed by the use of anti-aromatase drugs such as anastrozole.
When using testosterone propionate, aromatization is practically not expressed due to the short period of action of the steroid in the body.
Aromatization is not evil; aromatization increases the effectiveness of the AC course, since estrogens stimulate the production of IGF 1.
Aromatization “becomes evil” when the balance of sex hormones shifts towards estrogen. Estrogen levels are monitored using tests. But if you use propik, you most likely will not need them.
There is no need to specifically take anti-aromatase drugs and “kill” estrogen to zero; take them only if side effects occur.
If you have any negative effects of propionate on the liver, kidneys, gastrointestinal tract, heart, then there are no such negative effects!
As for the effect on the genitourinary system: Many people are interested in whether they will become impotent while taking testosterone propionate. They won't. On the contrary, during the course your libido will increase and you will feel like a “super man”.
Since propionate quite strongly suppresses the production of your own testosterone, after the course you may experience a slight drop in libido. In my practice, this only happened in the case of very long courses with large dosages of AC. By taking short courses on propionate - 6-7 weeks, you will most likely not even feel a drop in libido. Having carried out competent PCT, libido will quickly return to normal. Moreover, after the course, and taking tests, before the start of the course and after PCT, I more than once observed an increase in the level of my own testosterone, to values greater than it was before the course.
Pitfalls of testosterone therapy
26.04.2018
92242
3
In the next episode of the program “An Hour with a Leading Urologist” Stepan Sergeevich Krasnyak, employee of the Department of Andrology and Human Reproduction of the Research Institute of Urology and Interventional Radiology named after. N.A. Lopatkina of the Russian Ministry of Health, spoke about the problems associated with prescribing hormonal replacement therapy with testosterone drugs in men.
As Stepan Sergeevich noted at the beginning of his speech, the topic of testosterone therapy is extremely controversial and raises many questions among both doctors and patients. The prevalence of testosterone therapy today is growing rapidly, but the negative aspects of such treatment, according to the guest of the program, are often forgotten.
S.S. Krasnyak recalled the main areas of influence of testosterone on the male body. In particular, this hormone provokes the growth of body hair, is involved in the synthesis of whey proteins in the liver, causes enlargement of the penis and triggers spermatogenesis, affects thinking and mood, helps to increase strength and muscle mass, and from the kidneys is involved in the synthesis of erythropoietin, as well as supports bone growth in length and increase in their density. Accordingly, the less testosterone in the body, the less pronounced male sexual characteristics. Fortunately, according to Stepan Sergeevich, the decrease in the amount of this hormone is usually reversible.
Boundary between normality and pathology
It's no secret that testosterone levels tend to decline with age. However, is this process normal or pathological, and where is the line that allows us to distinguish between these two conditions? Most often, problems with testosterone occur in men over the age of 45–50 years. There are a number of criteria for identifying age-related hypogonadism. These include a decrease in serum testosterone (total <11 nmol/l, free <220 pmol/l), erectile dysfunction, decreased libido and decreased frequency of morning erections (EMAS data). The doctor emphasized that testosterone drugs are prescribed to treat not sexual dysfunction or obesity, but hypogonadism as such. The testosterone level threshold for prescribing hormone replacement therapy is 9.7–10.4 and 6.9 nmol/l.
Stepan Sergeevich noted the importance of a personalized approach to the patient: there are people with high receptor sensitivity in whom even low testosterone levels do not cause clear clinical manifestations. Accordingly, the question arises as to whether hormonal therapy is needed in such patients. Current clinical recommendations today indicate that, as a rule, it is not necessary. In practice, according to the lecturer, one must proceed from a combination of clinical symptoms, probably associated with low testosterone levels, and its laboratory confirmation. At the same time, it is important to avoid uncontrolled and excessive prescription/reception of testosterone.
In general, cases of symptom discrepancy (20–40% of the general population) and low circulating testosterone levels (20% of men > 70 years) are quite common. According to these criteria, only 2% of people aged 40 to 80 years have age-related hypogonadism and actually need testosterone therapy.
Hormone replacement therapy – billions of dollars
Today, testosterone replacement therapy is widely used throughout the world to treat hypogonadism and associated isolated symptoms. The alarming aspect of this trend, however, is that it has emerged without any serious scientific evidence regarding the benefits and risks of this type of therapy.
Today, injectable and gel testosterone preparations are mainly used. In the United States, sales of testosterone preparations between 2005 and 2010 has doubled and continues to grow. Similar trends can be seen all over the world. From 2000 to 2011, total sales of testosterone in the world increased 12 times to $1.8 billion. According to forecasts, in 2021, sales of testosterone preparations in the United States alone will amount to $3.8 billion. Inevitably, as Stepan Sergeevich noted, the question arises: is it really Have men become so much more likely to suffer from hypogonadism lately? It is possible that large scale overtreatment is occurring.
The doctor also spoke about the presence of scattered but numerous data indicating an increasing trend in the number of patients suffering from obesity associated with taking testosterone.
Replacement therapy, Stepan Sergeevich emphasized, should be offered to the patient only after a conversation that in the long term the beneficial and unfavorable consequences of this treatment for him are unknown. Thus, in 2021, at the Congress of the American Urological Association, a so-called urological “trial” was held, where, with the participation of practicing lawyers, a case of prescribing testosterone drugs to a patient with a high risk of cardiovascular diseases was examined, which ultimately led to his death. Interestingly, virtually no somatic diseases are contraindications to hormonal therapy. However, the doctor emphasized, this does not mean that it should be prescribed to everyone, including the most severely ill patients. Patients with a high risk of concomitant diseases must undergo specialized studies.
It is also noteworthy that many of the studies available on the topic today included men without symptoms of hypogonadism, while various testosterone thresholds, drugs, and dosage regimens were used for evaluation. Thus, it is very difficult to bring together data that would allow an objective assessment of the safety of testosterone therapy.
About pitfalls
At the very least, there are absolute contraindications for prescribing HRT. These include prostate and breast cancer, as well as liver tumors. Relative contraindications include prostate-specific antigen (PSA) level >4 ng/ml (or 3 ng/ml in men at high risk of developing prostate cancer); hematocrit >50%; severe lower urinary tract symptoms caused by benign prostatic hyperplasia (above 19 points on the IPSS scale); and poorly controlled congestive heart failure and sleep apnea.
There is some evidence that testosterone supplements increase prostate volume, ultimately causing a modest increase in PSA levels in older men. In 2005, the Journal of Gerontology published a report showing that the total number of prostate-related adverse events (prostate biopsies, cancer, serum PSA levels greater than 4 ng/mL, increased IPSS scores) was significantly higher in the group of patients those receiving testosterone than those receiving placebo (odds ratio 1.90; 95% CI 1.11–3.24; p<0.05). There are also data showing the results of testosterone supplementation in patients with locally advanced and metastatic prostate cancer (PCa). According to these data, in patients with aggressive and non-aggressive forms of the disease, the levels of total testosterone and sex hormone binding globulin were significantly different: in patients with an aggressive form of prostate cancer, testosterone levels were significantly higher. It is unclear whether we can talk about a cause-and-effect relationship here, but the fact of correlation has been revealed.
Another significant factor is hepatotoxicity. It is because of this that oral forms of testosterone preparations are prohibited in most countries today. Their use has been associated with the development of liver failure, benign and malignant liver neoplasms, intrahepatic cholestasis, hepatic purpura, hepatocellular adenoma and carcinoma.
In addition, a factor such as polycythemia was noted. A very common complication of taking testosterone drugs is erythrocytosis (hematocrit greater than 50%). Two meta-analyses performed in recent years have shown significant negative effects of testosterone therapy compared with placebo in this regard. There is a correlation between high testosterone levels and high hemoglobin levels. Erythrocytosis is more often dose-dependent and develops in older men during therapy with injectable forms of testosterone. The risk of such complications is especially high in the presence of other chronic diseases, for example, chronic obstructive pulmonary disease. Therefore, when prescribing testosterone drugs, control blood tests should be performed.
As for the effect of testosterone drugs on the cardiovascular system, this issue remains controversial. Due to the steady increase in cardiovascular mortality rates, it becomes especially acute. There is, in particular, evidence that testosterone intake correlates with the progression of heart failure, but the cause-and-effect relationship remains a matter of debate. The use of testosterone in coronary artery disease is thought to have a stimulatory atherogenic effect due to its negative effect on the lipid profile. However, normal physiological levels of testosterone have been shown to be beneficial for the male heart, and low levels are associated with an adverse risk of coronary disease outcomes. But, as S.S. Krasnyak emphasized, it is impossible to guarantee that a particular patient will achieve exactly the physiological level of testosterone without serious fluctuations.
In 2006, the New England Journal of Medicine published a study of 106 older men with a mean age of 74 years with low total testosterone, limited mobility, a high prevalence of hypertension, obesity, diabetes, pre-existing heart disease, and hyperlipidemia. For 6 months, patients underwent testosterone therapy in daily doses of 5 to 15 g. A placebo group was also allocated. The incidence of cardiovascular events was significantly higher in patients taking testosterone drugs (23% vs. 5%). Thus, Stepan Sergeevich summed up, it is impossible to assert the safety of such therapy, especially long-term therapy, in patients with existing diseases.
Testosterone and Fertility
Another serious issue is the effect of testosterone drugs on male fertility. There is evidence of a decrease in the volume of patients' testicles and a decrease in the number of sperm up to their complete absence (azoospermia) while taking testosterone drugs. In this case, the sperm count most often returns to its original level within 6 months after stopping therapy, but this does not always happen. This is especially important for young men, some of whom take hormonal medications to achieve rapid improvements in physical and athletic performance. Today there are even developments in the use of testosterone drugs as a means of male contraception.
Other factors
An important factor is also changes in the psyche: psychotic symptoms, excessive libido and aggression, in addition to physical and psychological dependence with withdrawal syndrome, quite rarely, but still noted by attending physicians in patients taking testosterone. In this sense, as the doctor noted, the hormone, like many things in the world, has dark and light sides. Taking testosterone may increase the patient's level of entrepreneurship and courage, but may also lead to aggression and suspiciousness. Here a lot depends on the innate qualities of the man himself.
A known side effect of testosterone drugs is gynecomastia. It is associated with the aromatization of testosterone to estradiol in peripheral adipose and muscle tissue. In this case, the ratio of estradiol to testosterone, as a rule, remains normal.
In addition, testosterone replacement therapy is associated with worsening sleep apnea. Its severe forms are a relative contraindication for therapy. In case of occurrence or exacerbation of obstructive apnea, a reduction in the dosage of the drug or discontinuation of therapy is required.
Like any anabolic steroids, testosterone preparations can cause nitrogen, sodium and water retention - the mineralocorticoid effect. Edema in such cases can worsen the condition of patients with heart, liver and kidney diseases.
The use of cutaneous forms of testosterone is associated with the phenomenon of hyperandrogenism in sexual partners of patients. Transdermal formulations may be associated with a range of skin reactions, mainly erythema and pruritus, which are also common with patch use. Intramuscular injections of testosterone, in turn, can cause local soreness and bruising.
Non-drug ways to increase testosterone
In addition to hormone replacement therapy, physical exercise, proper nutrition and regular visits to a urologist help maintain and increase testosterone levels at any age. Stress control also plays an important role. Many patients benefit from, for example, reducing their working hours. If there is a large volume of overtime work, the working day should be reduced to 10 hours. It is useful to spend at least 2 hours a day doing something you love that is not related to work: for example, reading or listening to music.
Regarding physical activity, there is a recent Japanese study (Kumagawa et al., 2015), which showed that after 12 weeks of high physical activity there was a significant increase in testosterone levels without hormone replacement therapy. Another study of 83 men (Trumble, Benjamin C. et al.) found that one hour of chopping wood increased testosterone levels by 48% (P < 0.001). Another work was carried out with the participation of 30 young men aged 18–27 years (Devi S. et al., 2014). They exercised on an exercise bike for 15 minutes a day with a heart rate of 125–150 beats per minute. After 12 weeks of such exercises, an increase in testosterone levels of up to 20% was observed.
There is also evidence that testosterone levels correlate well with waist circumference. Thus, getting rid of excess fat mass will in any case lead to an adjustment in the level of this hormone. It is weight loss that can be considered as a first-line therapeutic measure in patients with hypogonadism caused by obesity. There is a possibility that if weight loss is successful, the man will not need hormone replacement therapy in the future.
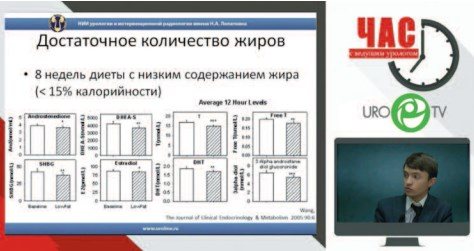
In the 21st century, prolonging life and maintaining its quality come to the fore among the tasks of medicine. Accordingly, patients should be given a number of simple recommendations that will help reduce the risk of developing metabolic syndrome and problems with testosterone levels. First of all, a man should change his diet and stop drinking excessively, and approach this systematically, and not as a temporary measure. However, the doctor emphasized, the patient does not need to be severely limited in the consumption of fats, including saturated fats: they are involved in the production of sex steroids, including testosterone. There is evidence of a strong correlation between high-density lipoprotein (HDL) levels and free testosterone levels (Heller, R.).
There are also a number of herbal remedies that have an evidence base for increasing testosterone levels. For example, 14-day consumption of Eurycoma longifolia extract has been shown to increase circulating testosterone levels by 30.2%. Another study found that the same extract increased the number of men with normal testosterone levels from 35.5 to 90.8%. In addition, 6-week consumption of Peruvian maca extract showed an increase in testosterone production by Leydig cells (Ohta Y. et al., 2016).
Stepan Sergeevich, however, noted that he understands the skepticism of some doctors regarding methods other than hormone replacement therapy. But, as he recalled, many of the active ingredients of the drugs synthesized today were initially obtained from plant materials. Therefore, the use of herbal remedies in addition to changing the amount of physical activity, adjusting diet and reducing daily stress levels may well bring results.
Stepan Sergeevich Krasnyak, employee of the Department of Andrology and Human Reproduction, Research Institute of Urology and Interventional Radiology named after. N. A. Lopatkina, Ministry of Health of Russia
The article was published in the journal “Urology Digest” No. 2/2018, pp. 26-34

Topics and tags
Testosterone
Comments

Oreshkov Vasily Sergeevich - 06.13.2018 - 17:42:36
Thank you very much for the informative report

Kiselev Evgeniy Alekseevich - 04/30/2018 - 11:14:14
I came across a statement that a new type of treatment undergoes damped fluctuations in assessment from “panacea” to “ineffective and harmful.” Over time, as application experience accumulates, a balanced position is formed. In the case of testosterone, these fluctuations are apparently far from dying out. Despite the fact that it has been used for about 80 years. Maybe non-medical factors intervene, artificially maintaining disputes?
Chernega Sergey Vasilievich - 04/26/2018 - 18:00:31
Thanks for the informative report
To post comments you must log in or register
What should I take testosterone propionate with?
Testosterone propionate is a universal, basic ester; in fact, it (or its long-living relatives) should be the basis for any course.
Combining it with other steroids is so widespread that there is no point in presenting all possible options within the framework of this article.
The only thing I would like to say is that propionate is not combined with other testosterones and testosterone mixes, for example sustanon. Why?
Yes, because the difference between these broadcasts is only in the duration of operation of one or another broadcast. The effect of application will be the same.
Propionate can be taken at the beginning of the course, for example, with testosterone enanthate, so to speak, for “acceleration”, until the long ester starts working at “full” power, followed by two weeks after the start of the course. Well, as mentioned above, it is also worth taking the drug as an “exit” from the cycle after long testosterone esters.
We will consider in detail the question of what you should take testosterone propionate with during a course separately, using the example of ready-made courses based on this steroid.