The Ministry of Health allowed cancer patients to participate in the Epivaccorona and Covivac studies
MOSCOW, April 14. /TASS/. Volunteers with cancer can take part in phase 3 clinical trials of Russian coronavirus vaccines Epivaccorona and Covivak to assess their effectiveness and safety for cancer patients. This is stated in the official response of the Ministry of Health of the Russian Federation to a request from Deputy Chairman of the Federation Council Committee on Social Policy Tatyana Kusayko (the document is available to TASS).
Earlier, Senator Kusayko sent a request to the head of the Ministry of Health of the Russian Federation, Mikhail Murashko, asking him to report on what work the department is doing to assess the effectiveness and safety of COVID-19 vaccines for cancer patients.
“When studying vaccines developed on the basis of traditional and fairly well-studied approaches (for example, an inactivated whole-virion purified vaccine or a vaccine based on synthetic peptide antigens of coronavirus proteins), volunteers with cancer can be included in a clinical trial. Currently, phase III clinical studies are being conducted to evaluate the effectiveness and safety of the Epivaccorona and Kovivak vaccines, in which volunteers with cancer can take part,” says the document signed by Deputy Head of the Russian Ministry of Health Oleg Gridnev.
As noted by the department, changes to the instructions for the medical use of vaccines against COVID-19 regarding the possibility of their use in relation to cancer patients can be carried out only after the completion of clinical studies with their participation and evaluation of the results. According to information provided by the federal scientific budgetary institution “Scientific Center for Expertise of Medicinal Products” of the Ministry of Health of the Russian Federation, the issue of the effect of vaccines for the prevention of COVID-19 on the course of cancer has not yet been sufficiently studied, the ministry emphasizes. “In this regard, the inclusion of volunteers with cancer in clinical trials of vaccines for the prevention of the new coronavirus infection COVID-19 depends on the type of vaccines and the knowledge of the platforms on which they are developed,” the letter says.
In early April, Director General of the National Medical Research Center of Radiology, chief freelance oncologist of the Ministry of Health of the Russian Federation, Andrei Kaprin, said that patients with cancer need to be vaccinated against the new coronavirus infection, but first consult with their doctor. Earlier, Kaprin also stated that specialists from the National Medical Research Center for Radiology of the Ministry of Health of the Russian Federation, together with scientists from the Center named after. N.F. Gamaleya prepared a general plan and description of methods for clinical trials of the vaccine against the new coronavirus “Sputnik V” on patients with cancer. The study will take six to seven months, he said.
Can cancer patients be vaccinated?
For patients with cancer, the issue of vaccination is very acute. Unfortunately, there is an opinion, including among doctors, that any vaccination is contraindicated for any malignant neoplasms.
Is it so?
No. Currently, a large number of large clinical studies have been conducted on this topic and their results have resulted in recommendations from the National Comprehensive Cancer Network (NCCN).
Why is such a misconception dangerous?
The patient is left without the protection that modern medicine can give him and is more susceptible to various infectious diseases, which can be very difficult and cause many complications.
similar on topic
Vaccination against COVID-19: can cancer patients be vaccinated?
READ MORE
What are the recommendations for vaccination of cancer patients?
The answer can be found in NCCN Guidelines Version 2.2020. Survivorship: Immunizations and infections.
The following vaccines are approved and recommended for use for all patients with cancer:
- inactivated or recombinant influenza vaccine;
- vaccines against diphtheria, tetanus, whooping cough;
- recombinant herpes zoster vaccine in all patients 50 years of age and older;
- HPV vaccine in previously unvaccinated adults under 45 years of age.
Recommended under special circumstances (for example, absence of a spleen, upcoming travel to an epidemic outbreak, epidemic situation):
- pneumococcal vaccine;
- hepatitis B vaccines;
- hepatitis A vaccines;
- meningococcal vaccine;
- vaccine against hemolytic fever type B, etc.
Introduction dates
Vaccines should be given 2 or more weeks before starting specific treatment and 3 or more months after finishing chemotherapy. Although this regimen is preferred, inactivated influenza vaccine may be given during cancer treatment if necessary.
Vaccines that are contraindicated or should be used with caution in patients with active immunodeficiency or used with caution in loved ones living and in contact with these patients:
- vaccine against measles, mumps, rubella;
- typhoid fever vaccine;
- live vaccine against herpes zoster;
- yellow fever vaccine;
- vaccine against rotavirus infection.
Introduction dates
Live viral vaccines can be given 4 or more weeks before treatment and 3 or more months after chemotherapy ends, but it is strongly recommended that you consult with an infectious disease specialist or physician familiar with vaccinating cancer patients.
In patients receiving anti-B cell antibody therapy, any vaccination should be delayed for at least 6 months after chemotherapy and the last dose of that therapy.
From these recommendations it is clear that the presence of cancer is not a reason to refuse vaccination completely. In the absence of contraindications, preventive vaccination is recommended to reduce the risk of developing infectious diseases.
References:
- NCCN Guidelines Version 2.2020. Survivorship.
- General recommendations on immunization - recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2011; 60:1-64. Available at: https://pubmed.ncbi.nlm.nih.gov/21293327/.
- Recommendations of the Advisory Committee on Immunization Practices for Use of Herpes Zoster Vaccines. MMWR Morb Mortal Wkly Rep/ January 26, 2021 / 67(3);103—108. Available at: https://www.cdc.gov/mmwr/volumes/67/wr/mm6703a5.htm.
- Human Papillomavirus (HPV) ACIP Vaccine Recommendations. Available at: https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/hpv.html.
- Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices - United States, 2020–21 Influenza Season. MMWR Recomm Rep. 2020 Aug 21; 69(8): 1–24. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7439976/.
Chubakova Galina Vladimirovna, oncologist surgeon, conducts personal consultations as part of our project for women who are faced with oncology. During the consultation, he will review your tests and research results, answer questions, and give recommendations for further observation.
PHOTOS: unsplash.com
We want to become even closer to you and will be grateful for your openness. To make our materials as useful and interesting to you as possible, please answer a few questions in the form at the link.
Share
Results
In connection with the announced launch of universal vaccination due to the coronavirus pandemic, many doubts and questions arise regarding the administration of the COVID-19 vaccine to cancer patients. Accordingly, questions arise about the validity, safety and effectiveness of immunization in cancer patients, including those receiving treatment.
There are currently no official studies conducted in these groups of patients. Still, experts say that the vaccine is safe for people who are in remission and receiving treatment aimed at strengthening the immune system.
What contraindications exist
If you have been diagnosed with leukemia or cancer, you should consult with your doctor before deciding to get a flu vaccination. In most cases, experts recommend getting vaccinated to reduce the risk of influenza during an epidemic. However, the final decision of the oncologist depends on the patient’s contraindications. Vaccination is prohibited if:
- a pronounced immune reaction to the previous vaccination,
- allergy to chicken protein,
- increased body temperature,
- runny nose, ARVI,
- insufficient kidney or heart function,
- immunodeficiency states,
- hypertension,
- diabetes,
- pathologies of the nervous system, adrenal glands, blood,
- age up to 6 months,
- diabetes,
- asthma.
Oncology refers to immunodeficiency conditions, and leukemia is one of the blood diseases, so it can be considered that vaccination cannot be carried out. The only absolute contraindication is leukemia. If you have an illness that affects other organs, you can choose the most favorable period and protect yourself from the flu. For tumors that have affected different organs, the date of vaccination is determined based on the stage of the chemotherapy course.
What to do for cancer patients during the coronavirus pandemic
Dmitry Yurievich, it’s especially difficult for cancer patients today. They must pass between Scylla and Charybdis. The new virus is dangerous, especially for people with such a serious disease, but oncology is not something to joke about. How can cancer patients live during a pandemic?
Dmitry Kanner, PhD, chief physician of Moscow City Oncology Hospital No. 62: All cancer patients can be divided into three groups. The first is primary patients in whom the tumor has been verified, confirmed, and is malignant, and the person must begin to be treated. According to research by our colleagues from Washington, and we are in touch with them, cancellation of treatment for such patients is much more dangerous than coronavirus.
Therefore, no matter how difficult the epidemic situation may be, oncology centers continue to work and treat - in compliance with all safety standards. The treatment tactics themselves do not change - surgery, chemotherapy, radiation therapy. Americans have already generalized that no one type of treatment - be it surgery, chemotherapy or radiation - is a more preferable method in the context of the coronavirus pandemic. It is important to comply with general epidemiological requirements.
We increased the space between patients, installed special machines with disinfectants at the entrance, masks again, and prohibited relatives from visiting sick people, explaining to people why this is important. In addition to organizational measures, for example, for endoscopic examinations, we introduced the use of a special plexiglass dome that isolates the patient from the doctors - we saw such a device from our Western colleagues and improved it. Treatment of cancer patients requiring emergency medical care is ongoing and does not stop.
On the other hand, if a person has been diagnosed with cancer that does not require urgent intervention, for example, tumors bordering on malignancy, skin tumors, basal cell carcinomas or small intestinal polyps, then we recommend that patients wait and postpone coming to the hospital.
The second type of patients are those whom the pandemic caught at the stage of treatment: chemotherapy, radiation therapy. Here you need to consider each specific case, whether it is possible to postpone the course. The point is not even that radiation, or, for example, intravenous infusion requires the presence of the patient in the clinic. And in the complications that treatment causes. These risks are weighed by the doctor on a case-by-case basis. For our part, we try to minimize the danger - for example, there are patients with prostate tumors or breast diseases who receive subcutaneous hormonal injections. We organized doctor-nurse teams to visit these patients at home, and judging by the gratitude from our patients, the decision was correct. I think that as soon as everything is over, we will take the initiative to consolidate this experience and make it everyday.
Finally, the third group of cancer patients is patients who have completed a course of treatment and who currently do not have obvious signs of the disease, but they need regular follow-up examinations, and if the disease develops, continued treatment. Such patients should definitely stay at home, in quarantine. Because the risk of getting an infection is very high, and if there are no complaints, you can wait two or three months. There are many such patients; they should follow all recommended measures for self-isolation, regimen and nutrition. And if you have any complaints, contact your doctor.
Oleg Ilyich, what would you advise cancer patients today? Not only as a scientist, a doctor oncologist with 55 years of experience, but also as a person who has gone through a serious cancer disease and continues to treat and teach.
Oleg Shcherbenko, leading researcher at the Federal State Budgetary Institution "Russian Research Center for Radiological Research" of the Ministry of Health of the Russian Federation, professor: Well, I got cancer fifteen years ago, what can I say now. I was treated for about six months, in cycles - chemotherapy, radiation. And during breaks I worked in the therapeutic department: if you are constantly busy, time flies faster. And in general, it is important that the matter is in hands. Then everything somehow went on an upswing. We must fight, oncology is not a death sentence, and now in a pandemic too.
Coronavirus is from the same group of viruses as influenza, respiratory viruses, that is, causing acute inflammation of the respiratory system. Only, unlike seasonal flu, the changes caused by coronavirus in the lung tissue are more severe. It has already been found that it damages the capillaries surrounding the alveoli - bubble-like formations of the lungs in which gas exchange occurs between the blood and the atmospheric air in the alveoli. Normally, red blood cells from the capillaries that surround the alveoli constantly absorb oxygen from the alveoli and release carbon dioxide there. But when the capillaries are damaged, liquid leaks out of them into the alveoli, the alveoli are filled with this liquid, and this disrupts the absorption of oxygen, so the person begins to choke, and then a microbial infection is added.
But the main difference of the new virus is that humans have not yet encountered a coronavirus of this type, which is why its contagiousness and degree of contagiousness are so high. And since it has recently been established that only a small number of people are immune to COVID-19, most people are at risk of getting sick. But how hard a person will endure infection depends on the body’s resistance, on its immunity. And since the population of the entire Earth does not have “herd immunity,” the decisive tools in defeating the virus can be two factors: the development of this “herd” immunity as a result of infection and recovery of the majority, or the creation of a vaccine. But this is a question for the future.
In the meantime, the picture is this: if a person is young, healthy, has no concomitant diseases, the body is able to resist, the infection can be asymptomatic, and such people will develop immunity - like those who have recovered from the disease. But if a person has health problems, for example, chronic diseases of the lungs, cardiovascular system, diabetes, the danger lies in the exacerbation of these disorders and even in a fatal outcome as a result of an exacerbation.
Now regarding cancer patients. It is generally accepted that their immunity is reduced. But this is a controversial issue. What kind of immunity? After all, there is humoral immunity, and there is cellular immunity. And in many cancer patients, the tumor is the result of a violation of local immunity, especially in young people. For example, a person has some kind of local tumor process, but neither cellular nor humoral immunity suffers, and such people are not susceptible to infectious diseases. But in the elderly or in those whose entire body systems are worn out, oncology can be a manifestation of the general state of the immune system. Therefore, it is impossible to say unequivocally: yes, for all cancer patients the risk of infection and fatal outcome is especially high.
But how can a person who has a tumor or has previously received treatment adjust their immunity so as not to get sick from coronavirus? In my opinion, any active intervention in the immune system, without knowing which link is broken and to what extent, can cause a negative reaction from the virus, which itself is immunogenic. The virus itself can cause some allergic reactions, already against the background of an altered immune system, excited by external factors. After all, when we take an immunostimulant and stimulate some sprout that may not need to be stimulated, this can lead to the development of a paradoxical allergic reaction with a severe course. Therefore, I consider stimulating the immune system of cancer patients with some external stimulants unjustified. General measures, yes - rational nutrition, lifestyle, physical and psychological hygiene, yes, this is all necessary.
Now regarding tactics: what to do if during a pandemic a person is suspected or diagnosed with cancer. Of course, go to oncologists for treatment, because if coronavirus gives one percent mortality rate, then for an advanced tumor the percentage is much higher, so you can’t waste time and let everything take its course, you have to go for treatment. Naturally, observing personal and social hygiene - distancing, masks, hand hygiene, and so on, the rules are common to everyone who is at risk of infection, and here they must be observed especially carefully.
If a pandemic overtakes a person while he is already receiving treatment, then it certainly needs to be continued, because, again, the risk from a tumor disease exceeds the risk from coronavirus disease.
If a person has already been treated for oncology, then all the rules recommended for ordinary people also apply to him - regardless of whether six months have passed since treatment, or all five. Here we proceed from the suspicion that the resistance of such a person may be lower than that of those who have never had cancer. But again, this is very conditional. Many effectively treated cancer patients do not have increased susceptibility to infections. And to say unequivocally: “Well, a person had a tumor, he was treated, and now he has suppressed immunity,” you can only look at his immunogram. It all depends on a person’s individual ability to recover, on the lifestyle he leads, on his desire to be healthy.
And there is nothing new here. Healthy lifestyle rules apply to everyone. Only if an absolutely healthy person who does not have a tumor can sometimes drink, and not get enough sleep, and work too much, and not eat enough, then for a cancer patient all these factors - malnutrition, overwork, lack of sleep, deprivation of fresh air - must be excluded. A nutritious diet with proteins, with the obligatory inclusion of fish, with limited carbohydrates, but with plenty of vegetables and fruits rich in vitamins, especially those with antioxidant qualities, and these are vitamins A, C, E, D and group B. Fats, of course, are not excluded , because the body needs cholesterol, but they should not predominate. For a patient with a tumor, moderate physical exercise is extremely important; walking is the most effective; staying in the fresh air is important. But if a person does not have a dacha, and he is forced to sit in self-isolation in an apartment, then he can, after all, at home, open the window or balcony, and run circles around the room.
My experience as an oncologist convinces me every day: in the fight for life, for your health, your attitude is important. Especially in oncology. What helps fight the disease? Thirst for life. The feeling that everything you were born for has not yet been done, that you have not yet completed something. A cancer patient must make plans for himself, and long-term plans at that. And go towards their implementation - purposefully. Don't sit idly by, don't wait for your death. If a person has some kind of goal, if he understands that he has not fulfilled his purpose, if he actively participates in the treatment process, then he will definitely recover and survive any viral infection.
How dangerous is COVID-19 for cancer patients?
To understand whether cancer patients can be vaccinated against coronavirus, we need to understand how dangerous the SARS-CoV-2 pathogen can be for this group of patients. Coronavirus infection is associated with a high probability of delays in cancer diagnosis, initiation of treatment, or long breaks in chronic treatment of tumor diseases.
Thus, even patients with uncomplicated COVID-19 may experience significant progression of the disease during the period of infection and remission. This, in turn, will result in some losing the chance for a full recovery, while others will never be able to return to effective cancer treatment.
Therefore, there is no doubt that COVID-19 poses a huge threat to cancer patients, not only due to complications of coronavirus infection, but also due to a significant increase in the risk of death from tumors. Therefore, vaccination against COVID-19 is an excellent opportunity to avoid both early and late consequences of infection and minimize the risks associated with cancer.
The COVID-19 vaccine, like the flu vaccine, does not contain “live” forms of the virus and does not pose a serious risk to the health of the person being vaccinated. The only side effects are inflammation at the injection site and allergic reactions.
Thus, as with the flu vaccination that is recommended annually for cancer patients, vaccination against COVID-19 should immediately become the standard of care in oncology, experts say.

Tomsk doctor on whether people who have had cancer can be vaccinated
TOMSK, October 10 – RIA Tomsk. People with and survivors of cancer need to be vaccinated against the flu, but this should only be done during the period of remission, Rimma Voloshina, head of the medical prevention department of the regional health department, told RIA Tomsk.
It’s not possible, but it’s necessary
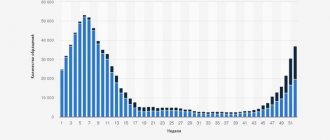
It was previously reported that influenza vaccination is underway in the Tomsk region. This year, Rospotrebnadzor plans to vaccinate at least 60% of the region’s population, which is 12% more than last year. In the new epidemic season, strains of influenza are expected that have not previously circulated in the territory, and therefore the importance of vaccination against influenza increases.
“This category of patients cannot, but need to be vaccinated against influenza: these people are prone to complications, so these patients must be protected. But the vaccine should be given not during the period of exacerbation of the disease, but during remission,” Voloshina said, answering a journalist’s question about whether cancer patients can be vaccinated.
According to her, in principle, for all patients, a contraindication for vaccination is an exacerbation of any disease. The vaccine can be given 2-3 weeks after the process has stopped. The specialist noted that it is especially important for pregnant women, people suffering from chronic diseases, and older people over the age of 65 to protect themselves from the flu.
“Elderly people are at risk, and we vaccinate this category at home. In city hospital No. 3, for example, about 2 thousand people were vaccinated at home. In total, all medical organizations vaccinated more than 8 thousand patients at home,” the specialist noted.
The vaccination campaign is in full swing
© RIA Tomsk. Pavel Stefansky

Seversk clinics are closing vaccination rooms due to the increase in COVID. She clarified that the vaccination campaign against influenza continues in Tomsk clinics. It is planned to be completed on November 1, so that immunity after vaccination has time to form before the epidemic rise in incidence. To avoid crowds of people, vaccinations are given by appointment; the flows of sick and healthy patients are separated.
“Vaccination against influenza is especially relevant in conditions of risk of spreading a new coronavirus infection; this is an opportunity to avoid cross-infection (coronavirus and influenza at the same time),” added the head of the department.
Previously, it was also reported, with reference to a representative of Rospotrebnadzor, that the list of contraindications to vaccination is small: an allergy to chicken protein, an exacerbation of a chronic disease or the presence of a disease in the acute period and a strong reaction to the previous administration of the vaccine. In other cases, if patients have any chronic non-infectious diseases, it is necessary to individually decide on vaccination with the treating doctor.
DO NOT EXPECT ANY EFFECT FROM SUPPRESSED IMMUNITY
— Chemotherapy and radiation therapy occupy a key place in the treatment of oncological diseases, along with the surgical method. Both of these types of treatment suppress all parts of the immune system (that is, they suppress it. - Ed.), explains the doctor. “As a result, the patient loses the specific immunity formed through vaccinations, in this case, the immunity developed after the coronavirus vaccine. The body becomes susceptible to infection, and the risk of mortality increases.
To date, a number of studies have already been conducted to assess the effectiveness of immunization of cancer patients with various “non-live” vaccines, notes Dmitry Baranovsky. There is no such data on anti-Covid vaccinations yet, but in terms of type, all three Russian vaccines are non-living - Sputnik V, EpiVacCorona from Novosibirsk, and CoviVac, says the expert.
— Maybe then “live” vaccines based on weakened strains of coronavirus are preferable for people with cancer? In different countries of the world, scientists are working on them.
— Such vaccines definitely cannot be prescribed to patients with weakened immune systems, since they can cause uncontrolled proliferation (that is, reproduction, growth. — Ed.) of viral particles in the body. Which will lead to a severe form of the disease. It is believed that the use of “live” vaccines in people with cancer is possible no less than 6 months after completion of chemotherapy and in the presence of stable remission.
Flu
Within a few days, the 2009 A/H1N1 swine flu vaccine will be available in your area.
Everyone has questions:
- Who will be vaccinated against swine flu A/H1N1 first?
- Is the swine flu A/H1N1 vaccine safe?
- Do I need to be vaccinated against swine flu A/H1N1?
- If I think I have had swine flu, do I need to be vaccinated?
- What is the difference between the nasal spray and the injectable form of the vaccine?
- I know that scientists say that vaccines preserved with thimerosal are safe, but is there an alternative?
- I heard that the vaccine contains a substance called squalene. This is true?
Here are the answers to these questions:
Who will be vaccinated against swine flu A/H1N1 first?
The nasal spray vaccine is approved for use only in healthy people aged 2 to 49 years. The first doses should be given to health care workers who have direct contact with patients and those caring for children under 6 months of age. (Young children are at high risk of developing complications from influenza but cannot receive the vaccine until 6 months of age.) The use of the vaccine in the form of a nasal spray in pregnant women is PROHIBITED.
Flu shots, depending on the manufacturer, are approved for use in children under 6 months of age and are safe for pregnant women.
Who should receive the vaccine first?
There are five such groups:
- Pregnant women are six times more likely to develop severe flu.
- Those who care for children under 6 months of age, including nannies. Young children are at increased risk of developing severe influenza and cannot be vaccinated until 6 months of age.
- Young people aged 6 months to 24 years who are most often affected by swine flu type A/H1N1.
- Medical workers and emergency personnel.
- Adults ages 25 to 64 who have conditions such as asthma that increase their risk of developing complications from the flu.
Is the swine flu A/H1N1 vaccine safe?
No vaccine is 100% safe for everyone.
The swine flu A/H1N1 vaccine, both a nasal spray and a shot, is created in exactly the same way as the seasonal flu vaccine.
Every year, the seasonal influenza vaccine, which includes a component of the seasonal influenza A virus, is changed to adapt to the virus changing its genotype. In the same way, a vaccine against the swine influenza A/H1N1 virus was created.
Long-term and short-term clinical studies are currently underway. Some results from short-term studies are already in: the vaccine does not cause any significant side effects other than soreness and redness at the injection site. About 10-15% of people feel tired or have a headache; Some may even experience a slight rise in temperature.
Also, even in people without visible allergies or sensitivities, the vaccine can cause more severe reactions, but this is rare.
And like the seasonal flu vaccine, the swine flu A/H1N1 vaccine should not be given to everyone. The vaccine is made from chicken eggs, so people with egg allergies should not receive this vaccine.
This vaccine is going to be administered to millions of people. There is a possibility that something bad could happen to some people around the time they get the vaccine. If they get into a car accident two days after receiving the vaccine, it is unlikely to be blamed on the vaccine.
Is it true that women have miscarriages soon after vaccination? There were frightening reports about this in the press. But experts convince people that events such as miscarriages are not so rare. It will take time to determine whether women who have been vaccinated are more likely to have a miscarriage.
It is very tragic that miscarriages occur every day in Ukraine. Some of them do happen some time after any vaccination.
Women, naturally, immediately begin to look for the most likely causes of this sad event, and often dwell on recent procedures, such as vaccinations. However, research shows that pregnant women who are and are not vaccinated against seasonal influenza have an equal chance of bearing a healthy baby unless the baby gets sick with the flu.
It's true that the H1N1 vaccine is new, but it was created using the same materials and processes as the seasonal flu vaccine. During clinical trials of the H1N1 vaccine, there was no risk of miscarriage in pregnant women (or other serious side effects). The Department of Health and Human Services and the Center for Disease Control have created a special surveillance system aimed at identifying currently unknown side effects of the H1N1 vaccine.
Pregnant women are at increased risk for developing serious illnesses if they become infected with influenza or seasonal flu, and this real danger threatening the expectant mother and her child outweighs all small and potential risks (which, by the way, does not include miscarriage). The CDC recommends that all pregnant women get both swine and seasonal flu vaccinations.
If vaccines are not 100% safe, why take the risk?
Authorized vaccines, including the 2009 H1N1 swine flu virus vaccine, are much safer than the diseases they may prevent. For example, for every million people who get the flu vaccine, one or two develop a severe neurological reaction called Guillain-Barré syndrome.
But the flu itself causes serious problems, including Guillain-Barre syndrome, in many more cases than two in a million. And since most of the population is expected to get swine flu, the risk of using the vaccine is much less than the risk of developing complications from the disease itself.
In clinical studies, 10,000–15,000 children and adults were vaccinated against H1N1 swine flu with drugs from various manufacturers. Nothing serious happened to any of them, including those who received a double dose of Sanofi-Pasteur's swine flu vaccine.
This does not prove that the vaccine will not cause harm. Clinical studies cannot determine whether something will happen to one or two out of 100,000 people vaccinated.
There is also the possibility of unexpected side effects. But according to the manufacturers, it is not great.
the 2009 H1N1 swine flu virus vaccine too new to
be trusted ? Is the swine flu vaccine a new development? Yes and no. The 2009 H1N1 swine flu vaccine is made in exactly the same way as the seasonal flu vaccine, by the same manufacturers and from the same substances, except for one new part.
A particle of the virus that is used in the vaccine to specifically activate the immune system has been changed.
Vaccine experts don't think the change is all that new. Every couple of years, a new variant of seasonal flu emerges. When this happens, a new vaccine is developed that uses the corresponding variant virus particle.
And even though the 2009 H1N1 swine flu virus is a completely new virus, it is still very similar to seasonal flu viruses. One of the vaccines contains particles of three seasonal influenza viruses and protects against seasonal influenza type H1N1, which is 75% identical in its antigenic structure to the 2009 swine flu virus, but this vaccine does not provide protection against pandemic influenza.
Last year, about 10 million people were vaccinated against seasonal flu. This may be reassuring, but it does not prove that something rare and unexpected cannot happen.
All this does not deny that the viral particle that was used to prepare this vaccine has never been used before. No scientific calculation eliminates the possibility that something unexpected might happen.
But it is believed that the likelihood of this is not high. But the likelihood that the vaccine will prevent the development of a serious disease and death is very, very high.
Next »
Vaccination against COVID-19: can cancer patients be vaccinated?
Coronavirus disease (COVID-19) is a potentially severe acute respiratory infection caused by the SARS-COV-2 coronavirus. The disease is caused by a new coronavirus, against which people initially do not have acquired immunity. There are many coronaviruses in nature, and we have been sick with many types of coronaviruses. But this type of virus appeared for the first time and therefore received the name - the new coronavirus infection COVID-19. So far, scientists cannot explain and find reliable reasons on which the severity of the disease depends. At the moment, a cure that can cure COVID-19 has not been found, but quite effective treatment regimens have been developed that have saved thousands of lives. Vaccines against COVID-19 have been developed in many countries, and when conducting vaccinations, doctors are currently guided by the “Temporary Guidelines of the Ministry of Health of the Russian Federation dated September 3, 2020.”
similar on topic
Can cancer patients be vaccinated?
READ MORE
At the time of writing, two vaccines have been registered and approved for use in the Russian Federation: SPUTNIK V and EpiVacCorona.
In the Russian Federation, on August 11, 2020, a combined vector vaccine was registered for the prevention of the new coronavirus infection COVID-19 in adults from 18 to 60 years old, Gam-COVID-Vac (SPUTNIK V), which induces the formation of humoral and cellular immunity against SARS-CoV-2 . The vaccine was obtained using a biotechnological method in which the SARS-CoV-2 virus is not used.
The drug consists of two components: a recombinant adenoviral vector based on human adenovirus serotype 26, carrying the SARS-CoV-2 S protein gene (component I) and a recombinant adenoviral vector based on human adenovirus serotype 5, carrying the SARS-CoV-2 S protein gene 2 (component II). The vaccine should be stored in a place protected from light, at a temperature not exceeding minus 18 °C. Storage of the thawed drug is allowed for no more than 30 minutes.
Vaccination is carried out in two stages: first, component I is administered in a dose of 0.5 ml, then after 3 weeks component II is administered in a dose of 0.5 ml. The drug is administered intramuscularly into the upper third of the outer surface of the shoulder, and if not possible, into the vastus lateralis muscle.
On the day of vaccination, the patient must be examined by a medical professional with a mandatory measurement of body temperature. If the body temperature rises above 37 °C, vaccination is not carried out.
After the vaccine is administered, the patient should be under the supervision of a medical professional for 30 minutes.
Vaccination should be prescribed with caution to patients diagnosed with:
- chronic liver and kidney diseases;
- severe dysfunction of the endocrine system (for example, diabetes mellitus);
- severe diseases of the hematopoietic system;
- epilepsy;
- stroke and other severe diseases of the central nervous system;
- severe diseases of the cardiovascular system (history of myocardial infarction, coronary heart disease, myocarditis, endocarditis, pericarditis);
- primary and secondary immunodeficiency;
- autoimmune diseases;
- lung diseases;
- metabolic syndrome;
- allergic reactions, atopy, eczema.
Persons who have not had COVID-19 and do not have antibodies to SARS-CoV-2 based on the results of serological studies are subject to vaccination.
Contraindications for the administration of component I of the vaccine are:
- hypersensitivity to any component of the vaccine or a vaccine containing similar components; history of severe allergic reactions;
- acute infectious and non-infectious diseases, exacerbations of chronic ones;
- diseases (vaccination is carried out 2-4 weeks after recovery or remission); for mild ARVI and acute infectious diseases of the gastrointestinal tract, vaccination is carried out after normalization of body temperature; pregnancy and breastfeeding;
- age under 18 years and over 60 years (due to lack of data on effectiveness and safety).
Vaccination can be given to patients who have received treatment for cancer and are in stable remission.
Cancer patients in remission for 5 years or more can receive the vaccine, following all the recommendations as for ordinary patients. For patients in remission less than 5 years old, the decision to vaccinate should be made individually after examination by a doctor. Patients currently undergoing treatment should not receive the vaccine.
Active development of new vaccines continues in Russia and other countries of the world. Indications and contraindications for vaccination are the same as given above.
According to these recommendations, at the moment there is no routine vaccination for cancer patients, but trials of a vaccine for cancer patients are being conducted on volunteers. The immune response of patients and the presence and frequency of possible complications are studied.
Oncological care, including surgical care, is provided in full. Operations should not be postponed to a later time. For elective surgery and chemotherapy and radiation therapy, patients who do not currently have symptoms of COVID-19 should be taken
.
This is confirmed by PCR analysis - a swab from the nose and throat, clinical symptoms and blood tests, including for antibodies to COVID-19. Refusals to perform operations on patients without signs of coronavirus infection are not justified, and patients should insist on the necessary treatment
.
We will further inform cancer patients about vaccination as new information becomes available, follow the news on the New Life website.
Kudinova Elena Gennadievna, head of the radiology department of the MD GROUP group hospital, oncologist, radiologist.
PHOTOS: NICEM im. N. F. Gamaleya
Share