Photo: medaboutme.ru
Victoria Mamaeva
Chief editor of Filzor. Specialist in the field of Pharmacy
Tatiana Senkina
Candidate of Medical Sciences, pulmonologist, phthisiatrician
Tuberculosis is one of the most terrible diseases of our world. Recently, in progressive countries, this problem has faded into the background in comparison with the epidemiological situation at the beginning of the last century, however, it has not been completely resolved.
You can protect yourself from the disease by vaccination with BCG . Short for Bacillus Calmette-Guérin , French - Bacillus Calmette-Guérin, BCG
.
Explanation of BCG vaccination
The BCG vaccine was obtained by Guerin and Calmette on the basis of bovine mycobacteria. Scientists subcultured this strain 230 times in an environment uncomfortable for bacteria, using bile and glycerol. Work on this began back in 1908.
It turned out that after 4 years the virulence for livestock disappeared. After 13 years from the beginning of the experiment, the elimination of virulence for monkeys and rabbits was revealed. The individuals who participated in the experiment received protection from mycobacteria - they were not afraid of infection in the future.
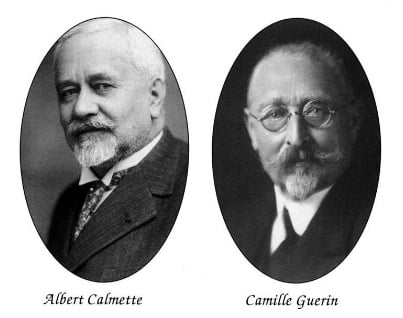
Albert Calmette (French: Leon Charles Albert Calmette) and Jean-Marie Camille Guerin (French: Jean-Marie Camille Guerin). Photo: estudiossocialesonline.com
Based on the results of many years of work, scientists created a strain named after them - BCG. In 1921, a child was vaccinated for the first time in France. The drug was administered orally.
Today, BCG vaccination and revaccination is included in the list of mandatory in 31 countries, and is recommended to the population in another 150. It is estimated that there are about 2 billion vaccinated people on the planet.
In the USSR, the medicine began to be used in 1926. In 1941, domestic scientists invented a dry vaccine. It could be stored for more than a year, while the liquid one used earlier retained its quality for only 2 weeks. This development has replaced the old form and is used by doctors to this day.
The BCG-M vaccine has also been developed , containing a smaller number of bacteria in 0.1 ml of the drug (compared to the first). Observations have shown that it is sufficient to create long-lasting immunity. BCG-M (decoding sounds like Bacillus Calmette-Guérin weakened) is used both for the first vaccination and for repeated preventive measures. Both in our country and in a number of CIS countries, BCG-M is the first choice vaccine for primary immunization. The incidence of side effects for such a drug is on average 5 times less in comparison with that inherent in BCG.
However, scientists do not stop improving the drug. Now the task is to completely abandon the use of living cultures. It is likely that in the future BCG will be replaced by a more effective and safe product created by genetic engineering methods, but for now the best protection against tuberculosis is the BCG vaccine.

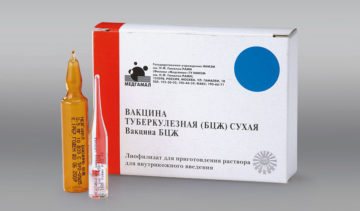
Tuberculosis vaccine (BCG-M). Photo: old.medach.pro
This is interesting: about the name! BCG is a reading of the foreign name BCG - an abbreviation for Bacillus Calmette-Guérin.
History of BCG
- In the USSR, compulsory vaccination of infants has existed since 1962. Russia has adopted this rule. Citizens of our country are also entitled to revaccination. Vaccination laws establish when BCG is given.
- In England, mandatory receipt of the BCG vaccine was adopted in 1953. Until recently, all children under 13 years of age, as well as infants at risk, were required to be vaccinated. Those in contact with tuberculosis patients were subject to vaccination. Statistics show that adolescents and young adults are the most vulnerable age group, and protection from immunization lasts no more than 15 years. The population of England was vaccinated en masse during the peak of the disease. Children over the age of one year are vaccinated en masse in England. Now the British are eligible for vaccination if they have risk factors. It is recommended to do BCG if you are planning a three-month (or longer) visit to a country with an unfavorable epidemiological situation.
- In India, mass use of the vaccine has been accepted since 1948. This country became the first non-European country to support this practice and appreciate how terrible it is that the BCG vaccine protects against.
- In 1967, Brazil also supported immunization of the population. The laws of the country oblige medical workers to regularly administer the BCG vaccine.
- In Germany, immediately after World War II, universal immunization was adopted. In those days, all German parents knew what the BCG vaccine would protect newborns from for many years. The practice continued until 1998, when compulsory vaccination was abolished on the recommendation of the Koch Institute. This was largely facilitated (as in England) by the favorable epidemiological situation. Selective immunization according to indications is now practiced, so parents have the right to choose whether to give BCG to their child.
- In Malaysia and Singapore, the vaccine was previously administered to infants, then again to 12-year-olds. At the beginning of this century, the regimen was revised and the drug is administered only once - when the child is born. The next vaccination after BCG is administered a month or later.
- Mass childhood vaccination is widespread in Latvia and Lithuania, Estonia for infants under one year of age. At the same age, children born in Bulgaria, Hungary, and Romania must receive the medicine. The practice is similar in Slovakia, where parents know exactly whether their children can go for walks after BCG (yes, they can). Children over the age of one year are vaccinated en masse in Malta and Norway. This practice is followed by Greece and France, where the administration of the BCG vaccine is mandatory.
- The Austrians and Belgians, the Danes, Italians and Spaniards abandoned mass immunization of children. This position is shared by doctors from Cyprus and Andorra, Sweden and Slovenia.
- Selective immunization of children is recommended in Switzerland, the Netherlands, and the Czech Republic. This practice is followed in Luxembourg. Although reactions after BCG are usually only local, the incidence of tuberculosis in these countries is so low that they become a sufficient reason to refuse the medicine.
Why is BCG revaccination necessary?
Bacillus Calmette-Guerin (BCG) can persist for a long time, provoking the development of immunity to tuberculosis. A couple of weeks after the vaccination is done, the strain turns into a specific L form that can remain in the body for a long time.
It has been noted that vaccinated children and adults are significantly less likely to develop tuberculosis.
The mortality rate among them is minimal . Immunity remains for 5-7 years. Therefore, after a while, re-vaccination is carried out.
Vaccine composition
The BCG vaccine contains 0.05 mg of microbial cells and a stabilizer - monosodium glutamate. There are no antibiotics or preservatives in the medicine. The kit usually comes with a solvent. This is sodium chloride, which is used to prepare the solution.
The instructions describe the BCG vaccine as a porous mass resembling powder or compressed into an openwork tablet. This is a hygroscopic substance. Many consumers are interested in what the BCG vaccination looks like. When diluted, it is a light liquid containing flakes. When the drug is administered, a vaccine strain of mycobacteria enters the body, which begins to reproduce and initiates the formation of long-term immunity.

BCG vaccine. Photo: diabetes-control.ru
Serious complications
Serious complications are rarely observed after vaccination. They cannot be regarded as a variant of the norm.
If the following changes occur, you should immediately seek medical help:
- Lymphadenitis of regional type . Inflammation of the lymph nodes is noted on the left side in the armpit area. An inflammatory process occurs due to the penetration of microbacteria present in the serum into the regional lymph nodes. The course of lymphadenitis is observed to a moderate degree. Accompanying it are signs of intoxication. Suppuration of the lymph nodes and the formation of fistulas are often observed. Therapy is carried out through surgery. The affected lymph nodes are excised.
- Local reactions are pronounced . Severe suppuration is possible, spreading beyond the injection site. The papule fills with pus and can burst on its own, forming a large, weeping area. As a rule, such changes are observed in the presence of primary immunodeficiency.
- Cold abscess . It has significant differences from suppuration. It appears on the skin several weeks after vaccination due to non-compliance with the rules for administering the drug. The injection must be given intradermally, but sometimes medical workers perform it intramuscularly, subcutaneously. A cold abscess does not cause pain. When it appears, the condition does not worsen. Negative changes are possible when it opens spontaneously and pus flows out.
- BCG osteomyelitis . It is considered one of the most dangerous complications. The skeletal system is affected. The pathological process develops slowly. Its first clinical manifestations can be noticed three months after immunization. As a rule, negative changes are observed due to the use of a low-quality drug or the presence of immunodeficiency.

Keloid scar . Occurs due to intradermal administration of the drug. The final formation of rough scars is recorded only a year after the vaccination. In an advanced form, it can continue to grow, causing itching and pain. The child should be constantly monitored by a phthisiatrician, pediatrician, and surgeon.

Extensive ulceration of more than ten millimeters . Indicates hypersensitivity to serum components. Its appearance is possible due to infection, ineffectiveness of the components of the medication.
- Generalized BCG infection . It is observed extremely rarely. Manifested by a complete lack of immunity. Occurs due to immunodeficiency.
Indications for vaccination
- infants born and living in areas with an unfavorable epidemiological situation;
- children, if they are at particular risk, live in low-endemic areas;
- persons who regularly come into contact with sources of mycobacteria.
In the latter case, this is especially true if the mycobacterium is resistant to classical drugs. With constant contact with patients, not only a one-time administration of BCG is indicated: repeated administration is necessary, and the frequency is determined based on the nuances of the situation.
Active prevention is carried out if the incidence of tuberculosis exceeds 80 cases per 100,000 people. If a child is surrounded by tuberculosis patients, he or she must be vaccinated with BCG.
To whom and when do they do it?
The Russian national vaccination calendar recommends that all healthy newborn children be vaccinated against tuberculosis in the first days of life.
Further, Mantoux tests are performed annually to diagnose tuberculosis and detect infection with mycobacteria in children. This is a subcutaneous injection of tuberculin - a filtrate of killed cultures of Mycobacterium tuberculosis that have undergone special treatment. After the test, redness or a papule (solidification) may appear at the injection site. The reaction to tuberculin is assessed by its size (Fig. 2). If the test is negative (there is no severe redness or swelling at the injection site), then the child is healthy, and the doctor may recommend revaccination.
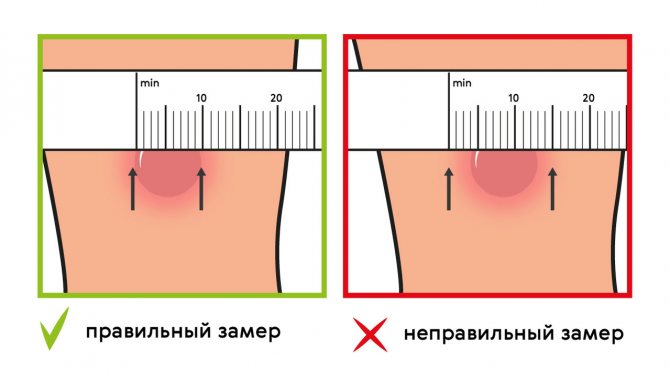
Figure 2. Assessment of response to tuberculin test. Source: MedPortal
Vaccination against tuberculosis can also be given to adults, but it is not as effective as in childhood. It is recommended to get vaccinated if a person is going to travel to a country with a high incidence of tuberculosis, or if he will have contact with patients. Vaccination is performed only if the tuberculin test gives a negative result.
Contraindications to vaccination
- severe immunity disorders;
- congenital immunodeficiency (including suspicion of such);
- leukemia;
- lymphoma;
- multifocal oncology;
- taking medications that suppress the immune system;
- pregnancy;
- the vaccine cannot be administered if the child is born premature and weighs less than 2.5 kg;
- the vaccine is not given due to intrauterine malnutrition (stages 3-4);
- if there are no tests for HIV of the mother during pregnancy, as well as the presence of a positive result of such a test. In this case, only at 18 months of age is the exact HIV status determined, after which a decision is made on the possibility of immunization. Although BCG vaccination is well tolerated after a year, it is recommended to change the drug to BCG-M;
- You cannot vaccinate a person during a period of acute illness or exacerbation of a chronic illness. In this case, the administration is postponed, waiting for recovery or remission;
- the reason for the withdrawal is severe blood diseases: BCG is either prohibited or postponed;
- if a person has received immunosuppressants or undergone a course of radiation, vaccination is done six months later or later.
This is interesting: a pregnancy exemption! There is no confirmed information about the dangers of immunization during pregnancy. Vaccination is not carried out due to established general practice.
Pediatricians did not notice tuberculosis
Soviet propaganda about a “bright, infection-free life through vaccinations” has done its job: more than one generation of doctors firmly believes in this utopia. And often a weakened, not yet recovered child is sent for the next vaccination, so as not to disrupt the vaccination schedule, determining “by eye” not only the readiness of the immune system to fight a foreign protein, but also... titers of specific antibodies. As a result, a new blow not only affects the cells of the immune system. All cells of the body react to the alien - foreign protein - antigen. The vicious circle closes. Vaccines literally restructure a person’s individual nature “in a general way.” This is a serious additional burden on the immune system, which is already wearing out prematurely in modern living conditions and in the dramatically changed human environment. The natural defenses of the body were not evolutionarily designed for the current loads plus the systematic artificial, aphysiological intake of foreign proteins... in case of “rescue”. As a result, secondary immunodeficiencies are acquired, often leading to paralysis of the immune system.
Today, despite “the most original system of vaccinations - everyone,” Russia occupies one of the first places in the world in terms of the largest percentage of children suffering from tuberculosis: annually about 2.5 thousand children (!) are registered with anti-tuberculosis dispensaries as patients with active form of tuberculosis (according to official documents).
Along with this, the warnings of old doctors about the increase in tuberculosis will come true if the vaccine against tuberculosis - BCG, which is especially dangerous during the neonatal period, is widely used. In February 1999, the symposium “Immunoprophylaxis of infectious diseases in children” of the Fifth Congress of Russian Pediatricians was held. It was about anything, but not about tuberculosis among vaccinated children. All academics and officials, who for decades had been assuring the world about “the victory and elimination of tuberculosis in a single country thanks to mass planned vaccination coverage of newborns,” at the congress tried to circumvent the topic of “victory” with the most incredible excuses. Pediatricians from all over Russia gathered, and not a word about childhood tuberculosis! Who are they lying to? Who is being deceived? Russia needs healthy children now more than ever. Nevertheless, this time IMMUNOPROPHYLAXIS was discussed without the participation of IMMUNOLOGISTS.
At the same time, for decades now there has been an internationally recognized contraindication to the administration of any live vaccines: immunodeficiency conditions - both primary (congenital) and secondary - acquired, as well as any other immunocompromised conditions. Who here determines these and other numerous contraindications to the administration of this or that vaccine?! And we have what we have: vaccination of immunocompromised children with a live vaccine against tuberculosis does not lead to protection from this infectious disease, but, on the contrary, to illness from it (of course, an exclusively susceptible group of people). Therefore, before vaccination, IT IS VERY IMPORTANT TO KNOW: IS IT NEEDED AND POSSIBLE to vaccinate a specific person, especially with a live vaccine.
Repeated vaccination
- revaccination cannot be carried out during periods of acute illness or exacerbation of chronic disease. This includes cases of allergies. BCG is used one month after recovery or remission;
- cancer;
- immunodeficiency; treatment with immunosuppressants, radiation (the entire period and six months after it);
- infection with mycobacteria;
- non-negative Mantoux test result;
- severe reactions to a previous tuberculosis vaccine;
- HIV infection.
If a person has received another vaccination, BCG can be administered a month after it - not earlier. An exception is the BCG vaccine “Imuron-vac”, used for bladder cancer.
Imuron-vac (BCG vaccine for the treatment of bladder cancer). Photo: poisklekarstv.com
Dangerous “small disease”
Let’s make it clear right away that the phrase “everyone in a row” is not ours. It is taken from the publications of pediatricians who promote the sanitary and epidemiological well-being of the population in Russia exclusively through vaccinations of “all children in a row.” If we take into account the publications of domestic specialists, among them, for example, neonatologist, academician V.A. Tabolin, then, starting from the 60s of the outgoing century, “practically healthy” newborns are practically absent. This has a lot to do with the health of children and adolescents, where the domestic system of irrational use of vaccines plays an important role.
When in 1948 they began to carry out total mass BCG vaccination in all urban and rural maternity hospitals, numerous specialists (pediatricians and phthisiatricians) expressed doubts about the harmlessness of such an event. BCG is a live antibacterial vaccine and cannot be indifferent to a highly susceptible contingent of people in whose bodies these vaccine mycobacteria must multiply, introducing “minor tuberculosis disease”. Given the imperfection of the immune system of newborns, an artificially created “minor disease” is unpredictable. In addition, BCG is a strong allergenic factor that can provoke any latent infection with which a child is born, transforming it into an active-acute form, which is completely undesirable during the neonatal period.
When conducting BCG vaccination among tuberculin-positive children, it was found that they were not vaccinated with the vaccine. This is explained primarily by the fact that these children already have a latent tuberculosis infection caused by either vaccine or other strains of mycobacteria, in the presence of which the administration of BCG does not produce the desired specific immune response. But the administration of BCG is also useless in the case when the child is not susceptible to tuberculosis.
It must also be remembered that a “tuberculin-positive” reaction can also be due to immunogenetic memory, which is passed on from generation to generation. Distant ancestors could have suffered from tuberculosis, but subsequent generations, even if they have never been sick, carry this immune-genetic inheritance within themselves and pass it on to their offspring.
In many countries around the world, tuberculosis vaccination is prohibited due to its danger and uselessness.
In Russia, it is also necessary to ban BCG vaccination for newborns. And the sooner we do this, the more we will save children from the consequences that are caused by live mycobacterium tuberculosis, from which this vaccine is prepared, taking into account the different susceptibility of each individual child to them. Post-vaccination complications, the abundance of which have been noted by pediatricians in the last half century, can also manifest themselves as long-term consequences months and years later: allergies, conjunctivitis, dysbiosis, otitis, nosebleeds, tonsillitis, bronchitis, pneumonia, bronchial asthma, inflammatory processes of the genitourinary tract, osteitis - disorders musculoskeletal system.
Consequences of BCG vaccination
A lot of controversy about the need for vaccination against tuberculosis is due to the fact that BCG relatively often causes side effects. As a rule, these are local reactions - swelling, redness, papule, small ulcer. It is possible to increase the temperature after BCG. During the initial administration of the vaccine, the reaction is observed after a month and disappears within 2-3 months, although deviations in the timing are possible.
If the BCG vaccination site turns red, there is no reason to panic. With repeated immunization, a local reaction is recorded in the first two weeks. The area must be protected from mechanical impact. On average, in 95% of cases, vaccination leads to the appearance of a scar (up to 1 cm) after BCG. In rare cases, more severe reactions have occurred.
Complications from vaccination
- lymphadenitis;
- ulcer;
- keloid scar;
- abscess;
- lupus;
- osteomyelitis;
- allergic syndrome.
The risk of death is estimated at 0.19 per million vaccinated. Almost always, the cause is the unintentional administration of a dose of BCG vaccine to a person whose cellular immunity is severely weakened. Regional lymphadenitis is almost always observed against the background of a very weak immune system. Infants have a higher risk of purulent lymphadenitis. To avoid this, use BCG-M. BCG is not administered to premature babies; the weakened version of BCG-M is always chosen.

Reaction to BCG vaccination. Photo: cgb-vuf74.ru
REACTIONS AND COMPLICATIONS DURING VACCINATION
In practice, most post-vaccination reactions are individual in nature and cannot be predicted. Most often, quite predictable mild reactions are observed at the injection site, expressed in swelling and redness of the shoulder and an increase in body temperature to subfebrile levels. Many of these reactions are caused by aseptic inflammation, often due to injection of the vaccine into the subcutaneous fat (especially when vaccinating obese individuals with a short needle). Such reactions go away on their own in a couple of days, and if you take paracetamol, then even faster. Sometimes there is an increase in regional lymph nodes - and this is also a normal reaction to the vaccine.

© ROBIN UTRECHT/AFP/Getty Images
The second most common reaction to vaccination is fainting. Often, from the very sight of the syringe or a few minutes after the injection, vaccine recipients lose consciousness, which is often accompanied by convulsions and vomiting. This reaction is of the same nature as fainting at the sight of blood. It is not related to the vaccine as such, but for an outsider, as well as for the person being vaccinated, such a reaction is very unpleasant. True allergic reactions to vaccine components are relatively rare, but after vaccination the patient should be monitored for an hour in order to react in time to possible anaphylaxis. Before receiving the vaccine, the patient must be asked about his allergies to the components of the vaccine (chicken protein in the influenza vaccine, baker's yeast in the hepatitis B vaccine, etc.).
It should be noted that the presence of contraindications does not mean that the vaccine recipient will inevitably experience a complication. However, contraindications protect the medical worker from possible legal consequences... A clever lawyer can prove to a judge, far from practical medicine, the connection between vaccination and a complication of pregnancy or the birth of a defective child. Therefore, pregnant women are not vaccinated against rubella, mumps, measles, chickenpox and BCG. But non-live anti-influenza vaccines began to be strongly recommended for pregnant women after the swine flu pandemic...
Do I need to get the BCG vaccine?
Back in 1935, trials began to confirm the effectiveness of the vaccine. The results of the work, which lasted until 1975, are ambiguous. The best results were observed in North America and northern Europe. In the tropics, low or no protection has been recorded. The reasons for this are the immunogenicity of the strains, genetic stability, as well as the specific influence of mycobacteria on humans depending on the climate. The bacilli that people encounter every day provide basic protection against mycobacteria. It, in turn, is strengthened by immunization. Ten studies were conducted that showed that the average protection of the live BCG vaccine against tuberculosis reaches 86%.
It's interesting: age plays a role! The reliability of vaccination is higher for newborns. The older the person, the less benefit from vaccination, since at the age of 10 years and older, tuberculosis is more often diagnosed in the secondary form.
Many people doubt the need for immunization, especially mass immunization. WHO specialists have released a special document, translated into many languages, explaining why the BCG vaccination is so significant. Among people aged 15-59 years, tuberculosis has the highest number of victims. Of the potentially fatal preventable cases, 26% are caused by it. In developing countries, young women most often die due to this disease, and not due to complications of pregnancy and childbirth. The incidence rate is regularly rising, especially in countries with poor living standards. Recent years have been marked by the emergence of drug-resistant mycobacteria. This significantly worsens the prognosis of treatment, while at the same time making the treatment process much more expensive. Administration of BCG to newborns is the best way to prevent the disease.
Doctors are sounding the alarm: over the years, bacteria will develop resistance to the antibacterial drugs of our time, and then to newer and more advanced ones. Of course, an improvement in the economic situation leads to a decrease in the incidence rate, but this takes decades. The only thing you can do right now is get immunized. It will not prevent the reactivation of a latent disease, and this condition is highly likely to lead to death, but BCG vaccination prevents infection in children and adolescents and saves thousands of lives across the planet.
The BCG vaccine is inexpensive and available all over the world. Administration of the drug may cause undesirable effects, but in general it is considered safe. Just one injection is enough. Of course, there are disadvantages, but immunization is currently a life-saving measure in many countries. Every year, about 100 million children receive their first TB vaccine. BCG is the oldest vaccine used in the world. It is not necessary to know what the abbreviation of the name means (its decoding), but everyone should know what the BCG vaccination is for.
Doubts about the need for vaccination are due to the risk of complications (more often at the site of administration of the BCG vaccine), as well as the improvement of the epidemiological situation in many countries. Unfortunately, everything is not so positive. Although the incidence rate is low in developed countries, atypical forms of the disease are increasingly being identified - the pathogen does not respond to medications. This forces us to re-raise the question of the need for mass vaccination, and doctors explain over and over again why and when they are vaccinated with BCG. The strains used by doctors come from the isolate created by Guerin and Calmette, but the work did not stop there. Over the past years, new strains have been invented that differ in phenotype and genotype. Largely because of this, it is difficult to list which BCG vaccines exist - there are quite a lot of them.
Since 1956, WHO has kept seed series to prevent new changes. The bacilli are extracted from the inoculum and cultivated under specific conditions, then filtered, concentrated, and diluted. The diluted preparation contains not only living bacteria, but also dead ones. None of the known strains have obvious benefits; everyone gives immunity after BCG. Scientists have not reached a consensus on the optimal strain that everyone should use.

Mycobacteria from the Mycobacterium tuberculosis complex group or Koch's bacillus. Photo: sharestory.me
Expert opinion on the importance of the vaccine
Answered by Senkina Tatyana Ivanovna, candidate of medical sciences, pulmonologist, phthisiatrician.
In 1921, in France, Calmette first used the BCG vaccine to prevent tuberculosis in a 6-year-old child. Further observations of this child for 5 years showed that he did not contract tuberculosis.
In the USSR, BCG vaccination began in 1926, initially as a scientific research.
By the thirties and forties, clinical observations of children vaccinated with BCG and a control group of children who did not receive the vaccine were completed. It was found that the incidence of tuberculosis among children who received the vaccine is 7 times less than among unvaccinated children. In addition, if there were cases of tuberculosis in vaccinated children, the forms of tuberculosis were uncomplicated with a favorable outcome.
Various methods of vaccine administration , including oral administration. In the course of scientific work, the most optimal method of administering the vaccine has been established - intradermal. Unfortunately, the vaccine had a short shelf life, making it difficult to transport within the country.
Since 1937, work began to find methods to extend the shelf life of the vaccine. In 1962, WHO approved the requirements for dry vaccine. Each country produces the BCG vaccine with different levels of viable mycobacteria involved in creating immunity. The Russian BCG vaccine (N.F. Gamaleya Research Institute of Epidemiology and Microbiology) contains 8 million/mg of live bacteria. The vaccination dose of the domestic vaccine contains 500-600 thousand bacteria capable of growing on nutrient media.
Clinical observations of the body's reaction to BCG vaccination are confirmed by data from pathomorphologists. The main changes develop in the lymph node system, reticuloendothelial apparatus of the liver, spleen and lungs. Changes in the body when the vaccine is administered begin in the first weeks after vaccination and increase after 3-4 months.
4-6 weeks after vaccination, a specific reaction develops at the site of intradermal injection of the vaccine in the form of an infiltrate with a diameter of 5-8 mm with a small nodule in the center. The nodule increases in size and turns into a pustule with caseous contents. The pustule may open, releasing a drop of thick pus - caseosis . A hemorrhagic crust forms over the opened pustule, under which caseation again accumulates. After 2-3 days, the crust is removed, a drop of caseosis is removed. And so on several times. Each time the crust becomes smaller in diameter, a post-vaccination scar is gradually formed. In some children (about 16% of all those vaccinated with BCG), a scar does not form, which is due to the innate characteristics of the immune system. But this does not mean that a child who received the BCG vaccine and who subsequently did not develop a post-vaccination scar is not protected from tuberculosis. Local vaccination reaction does not require any intervention. In children with normal immunity, the BCG vaccine does not cause any pathologies.
Currently, in addition to the BCG vaccine, the BCG-M vaccine for gentle immunization. This vaccine differs from the BCG vaccine in that the vaccination dose contains a smaller amount of dead microbial bodies, which helps reduce nonspecific allergic effects on the human body.
From 2021, it is planned to abolish revaccinations of BCG and BCG-M at 7 years and 14 years . That is, the child must be vaccinated against tuberculosis once, preferably in early childhood.
BCG: what is it?
The BCG vaccine is used to prevent severe forms of tuberculosis.
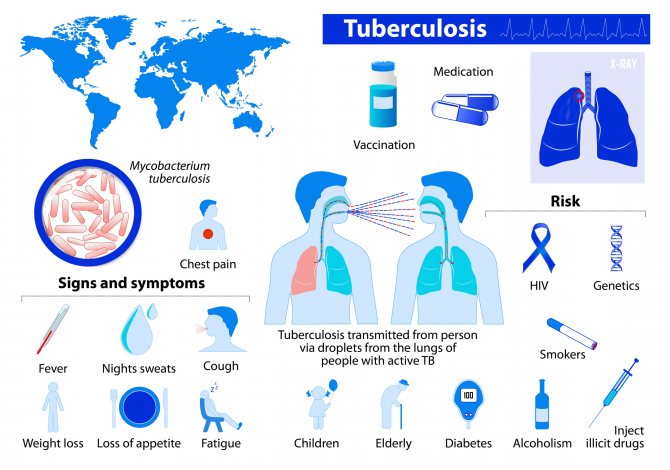
It also protects against the most dangerous complications if a person does get sick. Tuberculosis is a common infectious disease (Fig. 1). In the world, up to 10 million people fall ill with it every year, and up to 1.4 million people. dies from this disease. In Russia, the incidence of tuberculosis has been declining in recent years. In 2021 it amounted to 41.2 people. per 100,000 population, and mortality is 5.2 people. per 100,000 population. Despite this, tuberculosis infection remains dangerous, and BCG vaccination is important to protect against it.
Figure 1. General information about tuberculosis. Source:
The BCG vaccine is live. It contains live vaccine strains. They are obtained using weakened bovine tuberculosis bacilli Mycobacterium bovis.
M. bovis is a mycobacterium of the tuberculosis complex that can cause tuberculosis in humans in the same way as the main causative agent of the disease, Koch bacillus (Mycobacterium tuberculosis). Bovine tuberculosis bacillus and Koch's bacillus have a number of similarities and differences. M. bovis produces a similar immune response and can be weakened in vitro. This allows the strain to be used for the production of a live attenuated vaccine.
Back in 1908, the development of BCG began in France. The vaccine was named after the first letters of the surnames of its creators, Albert Calmette and Camille Guérin: Bacillus Calmette-Guérin or BCG. It was tested in 1921, but the tests were unsuccessful. Later it was transferred to the USSR. Since the 1950s, the mass use of BCG for vaccination began in the USSR and other countries. New vaccines are currently being developed, but for now BCG remains the only means of immunoprophylaxis against tuberculosis.
In countries where the incidence of tuberculosis is high, WHO recommends that all healthy newborns be vaccinated in the first days of life. Russia is one of such countries. In regions where the incidence of tuberculosis is decreasing or is low, vaccination against tuberculosis is carried out selectively, only for risk groups.
When is the vaccine given?
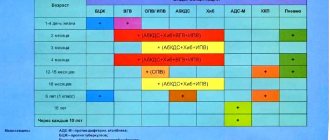
The tuberculosis vaccine is given 3-7 days after birth. Revaccination is indicated at the age of 6-7 years. Sometimes BCG is administered at one year or at another age, if there were reasons for withdrawal within the standard time frame. BCG vaccination after one year requires a preliminary Mantoux test.

BCG vaccination schedule. Photo: deskgram.cc
What to do if vaccination deadlines are missed
The vaccination calendar states that the child should receive the vaccine in the 1st week of life. A second BCG vaccination is also given at age 7. Due to various reasons (illness, etc.), withdrawal during this period is possible. This does not mean that vaccination is not needed in principle. The doctor will assess the patient’s condition, analyze the reason for the withdrawal, explain how many times BCG is usually given to a child, and choose a more appropriate time to give the injection, if there are no strict contraindications to this.
After vaccination
After vaccination you cannot:
- bathe the baby. This prohibition only applies to the day the vaccination was given. The next day, swimming is allowed;
- treat the vaccination site with various antiseptic agents. The healing of the vaccination is peculiar, the vaccination can fester and become covered with a crust, and many mothers ask whether it needs to be treated. There is no need to process anything, and it is very convenient; the graft heals on its own;
- rub the vaccination site;
- squeeze out the pus or tear off the crust at the vaccination site.
The BCG vaccination undergoes healing in several stages. This is a natural process and does not require any parental intervention. In 90-95% of vaccinated children, 5-6 months after vaccination, a small scar measuring from 3 to 10 mm forms at the injection site. This indicates successful vaccination and means that the vaccine worked and the child has developed immunity.
Where is the vaccine given?
The drug is administered intradermally. A single dose of BCG for children is 0.05 mg. To dissolve the powder, use 0.1 ml of sodium chloride.
Primary vaccination is usually indicated on the day of discharge from the hospital. If deviations are identified, vaccination is prescribed immediately after recovery. Usually, BCG is not used after the maternity hospital, giving preference to BCG-M. If the child is two months old or older, a Mantoux test must first be done. The personal card indicates the date of the event, the name of the vaccine, the manufacturer, its expiration date and the batch number. By the way, the opinion that you can’t bathe after BCG is just a common myth. The water is safe, but rubbing and scratching the area is really prohibited.
- The vaccine is sealed under vacuum conditions, so you must first cut the ampoule and only then break off the head. One ampoule contains 10 doses.
- Transfer 1 ml of liquid into the ampoule with a syringe and wait for dissolution for one minute. The finished product is a coarse suspension; color - white, grayish or slightly yellowish. It must be used immediately. Protect from light with a black paper cylinder. For diluted BCG vaccine, the shelf life is an hour.
- 2 doses of the vaccine are drawn into the syringe, half of the product is released with a needle, displacing the air. Having filled the syringe, they immediately give an injection.
- The BCG vaccine is administered intradermally. Zone - left shoulder, outer part, border of the first and second thirds.
- Pre-disinfect the area with alcohol.
- The bevel of the needle is inserted into the stretched skin. First, a very small amount of medicine is injected to check the correct position of the needle, then the rest of the volume is injected.
- If a white papule appears after injection, it means the injection was done correctly. After BCG injection, the size of the papule is up to 9 mm. The trail lasts for about half an hour. This reaction to BCG in a child is an absolute norm.
The risk of an abscess after BCG, when administered correctly, is minimal.

Where is BCG vaccination given to newborns? Photo: slide-share.ru
Ruler-diagnostician
Against the backdrop of the total mass coverage of BCG, every year from the age of one to 15 years, children undergo an intradermal Mantoux test, the same tuberculin test that we mentioned a little earlier.
The reaction to a tuberculin test combines two immunodiagnostic responses (completely incompatible in essence!): a) immunity to tuberculosis is assessed - 5 millimeters, and b) simultaneously - possible infection with mycobacteria (or tuberculosis disease - we have everything the same!) - 6 millimeters. Note that the difference is 1 millimeter... And this difference is determined... with a student’s ruler, which in itself is absurd!
It is necessary to remind and clarify: in our country, EVERYONE WHO RECEIVED THE LIVE BCG VACCINE during the neonatal period is infected (which, by the way, does not mean “sick”) with mycobacteria. It follows that everyone who is susceptible to tuberculosis to one degree or another and who has a “memory” of a violent encounter with mycobacteria - BCG - should have a positive response “to infection”.
Practice has shown that the tuberculin test (Mantoux test) cannot serve as a diagnostic tool after BCG vaccination. To establish the actual percentage of the population infected, this diagnostic test should be used BEFORE BCG VACCINATION. And immunity to tuberculosis is determined by other tests outside the human body. Anti-tuberculosis immunity does not depend on the presence of antibodies; what is important here is the result of the functional state of immunocompetent cells. And the “student ruler” method in this case is an outright falsification of this PREVENTIVE... help.
In addition, it is common knowledge that vaccinating does not mean protecting. The vaccine may not work, but the vaccinated person is considered protected, which also refers to the area of profanation. The result is important!
Experts from the WHO Ecology Committee, in contrast to the EPI Implementation Committee, having analyzed outbreaks of infectious diseases in different countries, came to the clear conclusion that infectious diseases recede (even without vaccinations!) with timely diagnosis, in the presence of high-quality water and a balanced diet. nutrition among the population, with the strictest EVERYDAY implementation of a set of anti-epidemic measures, which implies not only and not so much vaccinations... “The hope that an infectious disease can be defeated with the help of vaccines directed against this pathogen turned out to be too simplified, associated primarily with nature, properties and changing characteristics of pathogens,” WHO experts remind. In addition, other infectious diseases cannot be “defeated like smallpox,” each of which requires its own approach, its own program.
Preparing for vaccination
No specific measures are required. The doctor examines the child, checks the temperature. Parents give official voluntary consent.
In some cases, it is necessary to further examine the child or show him to a specialist. The need for such measures will be determined by the attending physician, who assesses the risks of complications after BCG vaccination.
If the child is older than 2 months, a Mantoux test must first be done, based on the results of which the possibility of immunization is determined. At the appointment, the doctor will explain how many days after Mantoux BCG can be administered without fear. The period ranges from 3 to 14 days.
There are no special rules regulating what to do after a BCG vaccination.
The introduction of other vaccines is allowed only a month or more after the BCG vaccination. If a person has received any vaccinations previously, at least a month must pass before BCG is administered. The exception is primary immunization against hepatitis B.
Features of vaccination
It is important to carry out vaccination against tuberculosis as early as possible, in the first few days after birth. This will allow you to activate your immune system faster. If immunization is performed later, BCG vaccination cannot be combined with other vaccines. One month before and one month after vaccination against tuberculosis infection there should be no other vaccinations. An exception is vaccination against viral hepatitis B, which is performed in the maternity hospital on the first day of a child’s life.
When using the BCG vaccine, the correct technique for administering the drug is especially important. It is injected to a certain depth, strictly intradermally. Incorrect injection depth provokes local complications and reduces the effectiveness of vaccination. It is better if the vaccination is administered by medical staff in the maternity hospital. Nurses in maternity hospitals constantly carry out such vaccinations and do them correctly, and in addition, the child will remain under the constant supervision of doctors for some time after vaccination. No special preparation is needed for BCG vaccination.
BCG-M vaccine
BCG-M is a gentle version of the BCG vaccine. One dose contains 0.025 mg of live bacteria. The halved number of bacteria is the main difference between BCG and BCG-M.
Indications for BCG-M
- premature;
- infants weighing less than 2.5 kg;
- children who are not immunized on time.
Vaccination with BCG-M is recommended instead of BCG for everyone if the epidemiological situation is consistently good.

BCG-M vaccine. Photo: khersonline.net
Contraindications to BCG-M
BCG-M cannot be used if the child weighs less than 2 kg, in case of acute illness, primary immunodeficiency, or cancer. The drug is contraindicated during treatment with immunosuppressants and radiation. The following are considered contraindications for the use of BCG-M:
- presence in the family of persons with generalized tuberculosis;
- Maternal HIV infection.
Side effects
After BCG-M, side effects are less common, but they are possible. Mostly these are local skin manifestations - swelling, redness, superficial scar.
Vaccination scheme
The effect of the vaccine is identical to BCG: the strain entering the body causes a cellular reaction, leading to the formation of long-term immunity. Immunization is indicated for newborns: BCG-M must be administered in the first week of life. Repeated administration is indicated at 7 years of age if a previously performed Mantoux test gave a negative result. If you did not get vaccinated in the first week, you can get immunized in the first 2 months of life without a preliminary diagnosis of tuberculosis. If more than 2 months have passed, you first need to do a Mantoux test.
The instructions for the BCG-M vaccine indicate the need for injection into the skin.
- The dose is dissolved in 0.1 ml of sodium chloride immediately before use.
- 2 doses are drawn into the syringe, the plunger is brought to the level of 0.1 ml and the drug is injected into the left shoulder (outer side).
- First, the skin is disinfected, then it is stretched, a needle is inserted, the correct insertion is checked, and all the medicine is released from the syringe. This leads to the appearance of a standard reaction to BCG-M: a white papule about 9 mm in diameter. Normally, it disappears in the next half hour.
Scheme of administration of the BCG-M vaccine. Photo: yandex.ru
Types of vaccines and features of vaccination
There are two types of tuberculosis vaccines available..
- BCG vaccine.
- BCG-M vaccine.
The tuberculosis vaccine is traditionally given in the upper third of the left shoulder. The BCG vaccine is administered only intradermally. The dose of one vaccination is 0.05 mg, it contains 0.1 ml of vaccine. Although it is very small, it is necessary to strictly follow the dosage, because the vaccine is a strong microbial agent, violation of the administration technique and dosage can cause complications after vaccination.
The injection technique for BCG-M is exactly the same, only the dosage is different: 0.1 ml of this vaccine contains only 0.025 mg of the active drug.
For vaccination and revaccination, both types of vaccine are used: BCG and BCG-M .
The vaccination is given to all healthy born children before discharge from the hospital, who have no contraindications. This usually happens on the 3-7th day after the baby is born. The vaccination is done in the morning, in a room specially designed for this purpose, only after examination by a pediatrician and in the absence of contraindications.
A note is made in the developmental history of the newborn, indicating the date of vaccination, as well as the vaccine series. These data, along with the discharge statement, are necessarily transferred to the clinic where the baby will be observed, and the local pediatrician enters them into the child’s record.
On the day of vaccination, you should not bathe your child. Usually the day of vaccination coincides with the day the mother and child are discharged from the maternity hospital, so the mother is warned about this in advance before vaccinating the baby. The day after vaccination, you can safely bathe your baby.
If in the family where the child was born there is a relative with tuberculosis, then the vaccinated newborn must be isolated for a while until immunity is developed. On average it takes 6-8 weeks. All pregnant women living next to a sick relative are registered with a TB doctor. They are monitored more closely as there is a risk of infection.
The gynecologist and pediatrician must be aware in advance, because the newborn must be isolated; the baby can be discharged only if the sick relative is hospitalized in a specialized hospital or after he is sent to a sanatorium for 2-3 months and the home is disinfected.
If all conditions are met, the mother and child are allowed to be discharged from the maternity hospital.
Conclusion
Although there has been a lot of debate lately about the need for vaccinations in general and the prevention of tuberculosis in particular, most doctors believe that vaccination is vital. Many reputable scientists speak out for and against BCG. Much depends on the epidemiological situation in the area of residence, but it should be remembered that even in a prosperous area there is a danger of infection. In unfavorable conditions, it is unacceptably high, and a vaccine is the only measure to prevent a serious illness.
Undoubtedly, the arguments of opponents are no less compelling: the use of the BCG vaccine provokes adverse reactions. Although they are very rare, the risks remain. If they are comparable to or higher than the risk of contracting tuberculosis, if the medical policy in the country and the peculiarities of the epidemiological situation allow it, you can refuse vaccination. In some cases, no arguments can outweigh the benefits of long-term protection against tuberculosis.
When not to use the drug
In addition to contraindications, employees of medical institutions may reject the entire batch or individual ampoules of the drug if:
- The vaccine has expired;
- There is no marking on the label;
- The ampoule is damaged, there are cracks on the body;
- The naked eye can see that the vaccine has changed its properties;
- The seal of the packaging is broken;
- Violation of vaccine transportation rules.
Shelf life of BCG
The drug should be stored in a cool place at a temperature of 0 to 8°C for no longer than two years.
After vaccination it is recommended:
- Do not treat the injection site with any disinfectants. This applies to any reactions to the vaccine (infiltrate, abscess, button, ulcers, etc.)
- Do not scratch, wash or touch the injection site;
- Sit for half an hour near the doctor’s office after the procedure (this is done in order to provide first aid in a timely manner in case of sudden complications);
- If there are any incomprehensible reactions of the body, inform your doctor;
- read the order of the Ministry of Health of Russia No. 109 “On improving anti-tuberculosis measures in the Russian Federation” dated March 21, 2003.”