An alternative to the Mantoux test for children can be Diaskintest with a lower dose of more purified tuberculin; allergies to it are less common. Instead of such skin tests, a blood test is taken - PCR (polymerase chain reaction) for the DNA of the tuberculosis bacillus. It is also suitable for examining a child before entering kindergarten, but it is not carried out in every laboratory.
Quantiferon analysis is very sensitive and specific, but it does not provide a 100% guarantee of the absence of infection, since it does not show the earliest stages of infection. The T-spot blood test is very similar to it. The most reliable way to confirm the pulmonary form of infection is an x-ray, but it is useless immediately after infection and will not show the risk of the disease.
When you need an alternative to Mantoux for children, what is it?
An alternative to the Mantoux test for children is necessary if there is intolerance to the components of tuberculin used for this test. The most common methods that a doctor may recommend to identify or rule out tuberculosis are listed in the table. They differ in specificity (the ability to detect tuberculosis infection) and sensitivity (the ability to make a diagnosis at an early stage).
| Method name | Specificity | Sensitivity |
| Diaskintest | 86% | 94% |
| T-spot | 84% | 42% |
| PCR (polymerase chain reaction) | 78% | 91% |
| Quantiferon test | 96% | 89% |
| Chest X-ray | 89% | 94% |
For comparison: the Mantoux test is quite specific (87%), but not very sensitive (65%). All methods for detecting tuberculosis infection are not 100% reliable, so they are used only in conjunction with studying the patient’s medical history, examination, and x-ray examination of parents (fluorography).
We recommend reading about the age at which Mantu is made. From the article you will learn how often the Mantoux test is done in kindergarten and school, the test schedule, and alternative diagnostic methods in older age. And here is more information about the dangers of large papules after the Mantoux test.
What can be used legally
By law, you can undergo any of the methods for diagnosing tuberculosis for a child. Parents may refuse to perform the Mantoux test, but most often this should not be done without reason. Usually the reason for changing to another method of examination is an allergic reaction to tuberculin. Then the doctor usually does not recommend the closest analogue - Diaskintest. It is best to conduct one of the blood tests: quantiferon test, T-spot, PCR.
Will they take me to the garden with an alternative sample?
The Mantoux test is suitable for kindergarten in a new way, that is, its closest analogue, its name is Diaskintest. They are very similar in principle and assessment. Before entering the children's team, a certificate from the local pediatrician is required, and he takes into account any of the examination methods.
How else to test a child for tuberculosis without Mantoux, what tests to take
There are several other ways to check a child for tuberculosis without Mantoux:
- Radiography is a fairly informative research method, but is absolutely not suitable for young children. It negatively affects the child’s development process, therefore it is prescribed only in exceptional cases. X-ray shows existing lesions in the lungs, does not reveal other forms of the disease, and gives an almost instant result.
- Quanteferon test - has no contraindications, is completely safe, provokes a response of the immune system to tubinfection. A positive test result does not always confirm the presence of infection in the body, and a negative test result does not at all exclude active disease. Can be used to diagnose the latent form of tuberculosis and immediately after BCG placement. The reliability of the result is 99%, but there is also a high probability of receiving an erroneous answer.

- The Suslov test is a blood test suitable for diagnosis in children with a history of allergies and at a young age. The test is absolutely safe, but has low sensitivity to antibodies. It is considered rare, and a disease localized in the lungs is almost impossible to detect using this method.
- Diaskintest - based on the reaction of the skin to a specific tuberculosis protein, is considered a complete analogue of the Mantoux test, but as improved as possible. Doctors evaluate the result after 72 hours - they measure the diameter of the papule. The method is simple, accurate, but has a high probability of obtaining a false negative result.
- Ziehl-Neelsen technique - the patient donates saliva for testing. The analysis is complex and involves several chemical reactions. It is safe and can be performed in case of existing allergies and chronic internal pathologies. The result will be a simple recording of the presence of Koch's bacillus without a clear definition of the stage of the disease and localization.
We recommend reading about whether it is necessary to make Mantoux. From the article you will learn when and why Mantoux is made, whether it is necessary to use it for kindergartens and schools, when you don’t have to do a test. And here is more information about how to write a refusal from Mantoux.
The Mantoux test is not the only method for diagnosing tuberculosis; parents have the right to choose blood tests. Their results can be used for admission to school and kindergarten, in most cases they will be more reliable.
Blood test instead of Mantoux
Blood tests are used to detect tuberculosis at an early stage; they can be prescribed instead of Mantoux to a child or together with a sample to clarify the diagnosis. The tests are called:
- PCR – detects the DNA of the tuberculosis bacillus;
- quantiferon - examine the level of interferon produced by cells of the immune system (T-lymphocytes) that have been in contact with the mycobacterium;
- T-spot - the number of T-lymphocytes in the blood that have reacted to the tuberculosis bacillus is counted.
Advantages and disadvantages
The most important advantage of blood tests is that they can be performed without the need for tuberculin administration. The disadvantage is the inability to identify what exactly is happening in the body - the active development of an infection or a harmless carriage of mycobacteria. Therefore, they cannot be considered the “gold standard” for detecting tuberculosis, and so far there are no such methods.
What makes it difficult to evaluate results is:
- reduced immunity;
- early period after infection;
- improper blood collection and transportation to the laboratory;
- erroneous assessment of the results.
The disadvantage is the need for special equipment, so such tests are carried out in large diagnostic centers. They have a high cost - above 5,000 rubles.

Carrying out PCR diagnostics of tuberculosis
From the point of view of reliability, blood tests can be used in countries with a low incidence of tuberculosis, but for Russia they are less informative. Out of 100 carriers of the infection, only one develops the disease, so the risk detected by the tests is exaggerated.
What is more effective
Currently, there are not enough blood tests for tuberculosis, so there are no accurate statistics on their effectiveness. It is believed that they should be used in combination with skin tests. The independent value of blood tests is lower than Diaskintest and the Mantoux test for identifying the risk of developing tuberculosis infection.
Diaskintest - an alternative to Mantoux
22.Mar.2019

Tuberculosis is an infectious, specific, chronic disease caused by Mycobacterium tuberculosis complex.
The natural reservoir of mycobacterium tuberculosis is humans, domestic and wild animals, and birds. The main mechanism of infection transmission is aerogenic (airborne). However, other routes of infection are possible: contact, nutritional, and most rarely vertical (from mother to child). Tuberculosis in children most often develops during primary infection with Mycobacterium tuberculosis (MBT). Of particular importance when children are infected with MTB is direct long-term contact with relatives with tuberculosis (parents, grandparents, aunts, uncles, etc.).
Tuberculosis (TB) is one of the most widespread infections in the world. According to the World Health Organization (WHO), a third of the world's population is infected with Mycobacterium tuberculosis. Every year about 9 million people fall ill with tuberculosis, and 1.5-2 million people die from tuberculosis.
TB is one of the three leading causes of death in women aged 15 to 44 years. In 2014, approximately 1,000,000 children became ill with tuberculosis, and 140,000 children died from tuberculosis.
In the Russian Federation, the share of children is about 5.0% of all cases of tuberculosis.
Options for the development of the situation after the penetration of the tuberculosis pathogen into the human body are as follows:
- complete elimination (removal) of MBT from the body;
- development of primary tuberculosis (with rapid growth and reproduction of the office)
- infection or “latent infection” (with the persistence of the office, which is in a dormant or “dormant” state), which can either remain so throughout life, or develop into a clinically manifested disease (with intensive reproduction of the office, ineffective immunity, etc.).
From the moment mycobacteria are introduced into the body, during the first year the disease develops in 5% of infected people; during the rest of their lives, tuberculosis develops in another 5%, i.e. The lifetime risk of tuberculosis among those infected is 10%. The presence of various factors may increase the risk of developing local tuberculosis. Thus, in the presence of HIV infection, the annual risk of developing tuberculosis due to LTBI is 10%, and the lifetime risk is 50%.
Risk factors for tuberculosis: contact with people with tuberculosis - close family, close apartment, industrial (at work, school), accidental, contact with animals with tuberculosis, lack of vaccination against tuberculosis (BCG, BCG-M), concomitant chronic diseases - urinary tract infections, chronic bronchitis, chronic purulent-inflammatory diseases of the respiratory system, diabetes mellitus, anemia, psychoneurological pathology, diseases requiring long-term cytostatic, immunosuppressive (including genetically engineered biological drugs) therapy (more than one month), primary and secondary, HIV infection, frequently ill children, young age (from 0 to 3 years), prepubertal and adolescent age (from 13 to 17 years), alcoholism of parents, drug addiction in parents, stay of parents in prison, unemployment of parents, homelessness children and adolescents, children ending up in orphanages, orphanages, social centers, etc., deprivation of parents of parental rights, migrants, refugees, etc.
Clinical manifestations:
A. Symptoms of inflammatory disease of the respiratory system (respiratory symptoms):
• prolonged cough (more than 2-3 weeks) with sputum production;
• chest pain;
B. Intoxication symptoms (more than 2-3 weeks):
• increased body temperature, often to low-grade levels;
• weakness;
• increased sweating, especially night sweats;
• weight loss (more than 10% of ideal), etc.
If at least one symptom is present, an examination is recommended to completely exclude suspicion of tuberculosis.
The absence of clinical symptoms does not exclude the disease.
In more than 50% of cases, tuberculosis in children is asymptomatic, therefore the main method for detecting tuberculosis infection (tuberculosis) in children is tuberculin diagnostics (immunodiagnostics), based on identifying delayed-type hypersensitivity in response to the presence of mycobacteria in the body.
Preventive medical examinations of the population are aimed at the timely detection of tuberculosis and are carried out in medical institutions at the place of residence, work, service, and study.
Conventionally, mass and individual immunodiagnostics are distinguished. Objectives of mass immunodiagnostics (screening for tuberculosis): detection of infection with Mycobacterium tuberculosis; selection of persons for vaccination and revaccination against tuberculosis; formation of risk groups for tuberculosis.
Objectives of individual immunodiagnostics: differential diagnosis of post-vaccination immunity (BCG) and true infection with Mycobacterium tuberculosis; differential diagnosis of tuberculosis and other diseases.
In the Russian Federation, it is recommended to conduct mass examination (screening) of the child population for tuberculosis infection (including when children enter educational organizations - in accordance with paragraphs 1, 2, part 2, article 23 of the Federal Law of December 29, 2012 No. 273-FZ “On education in the Russian Federation”). The examination is carried out annually by the method of immunodiagnostics at the age of 1 year - 17 years inclusive and by the method of fluorographic examination at the age of 15-17 years. In groups at high risk of tuberculosis, screening is recommended twice a year.
A necessary precondition for medical intervention (including intradermal administration of drugs) is the giving of informed voluntary consent of a minor or his legal representative to medical intervention (Article 20 of the Federal Law of November 21, 2011 No. 323-FZ “On the fundamentals of protecting the health of citizens in the Russian Federation”). Federation").
Immunodiagnosis of tuberculosis is carried out using an intradermal Mantoux test with 2 TE PPD and an intradermal test with the recombinant tuberculosis allergen (ATR or Diaskintest), developed in Russia in 2008, which is a complex of recombinant proteins CFP-10 and ESAT-6, intended for intradermal administration. The intradermal test with ATP has the highest sensitivity (98-100%); the highest specificity (90-100%); lack of development of a positive reaction associated with BCG vaccination; minimal frequency of manifestations of nonspecific allergies. The technique for performing an intradermal test with ATP is identical to performing the Mantoux test.
Immunodiagnosis is carried out for children vaccinated against tuberculosis from 12 months of age until they reach the age of 18 years. An intradermal allergy test with tuberculin (Mantoux test) is performed once a year, regardless of the results of previous tests up to and including 7 years of age. An intradermal allergy test with ATP is performed once a year, regardless of the results of previous tests from 8 years of age to 17 years of age inclusive. For those not vaccinated against tuberculosis, a Mantoux test is performed 2 times a year, starting from the age of 6 months.
Children from high-risk groups for tuberculosis who are not subject to dispensary registration by a phthisiatrician, patients with diabetes mellitus, peptic ulcer disease; patients with chronic nonspecific purulent-inflammatory diseases of the bronchopulmonary system and kidneys; patients with HIV infection; patients receiving immunosuppressive therapy for a long time (cytostatics, corticosteroids, genetically engineered biological drugs (GEBP), etc.), an ATP test is carried out 2 times a year in medical organizations of the general medical network. If necessary, perform a Mantoux test with 2 TE PPD-L. Simultaneous testing on different hands is allowed.
It is not recommended to carry out only a test with the recombinant tuberculosis allergen (without the Mantoux test) for children under the age of 7 years inclusive. The Mantoux test is necessary to select individuals for BCG revaccination (6-7 years old)
Based on the results of immunodiagnostics, for further examination in order to exclude tuberculosis and diagnose latent tuberculosis infection, children are referred to a phthisiatrician for consultation within 6 days from the date of the Mantoux test.
If a child is referred to a TB specialist, it is recommended to conduct a fluorographic examination of the child’s environment if more than 6 months have passed since the last examination.
Children referred to a TB specialist are recommended to undergo additional examination methods: general blood and urine tests, radiation examination methods
A positive result for an ATP test suggests the presence in the patient’s body of a population of actively metabolizing MBT, which can lead to disease. In this regard, it is recommended for all patients with positive results for the ATP test to have a computed tomography (CT) scan of the chest organs to confirm or exclude tuberculosis of the respiratory system (intrathoracic lymph nodes, lungs).
A refusal to examine a child for tuberculosis infection must be formalized in writing by the child’s legal representative and filed with the child’s medical documentation (form No. 112/u, 026/u-2000 (Clause 7, Article 20 of the Federal Law of November 21, 2011 “ On the fundamentals of protecting the health of citizens in the Russian Federation "No. 323-FZ). If a citizen, one of the parents or another legal representative refuses medical intervention, the possible consequences of such refusal must be explained in a form accessible to him (clause 4 of Article 20 of the Federal Law dated November 21, 2011 “On the fundamentals of protecting the health of citizens in the Russian Federation" No. 323-FZ). If the legal representative refuses to formalize a written refusal, a corresponding entry is made in the child’s medical records and sealed with the signatures of two medical workers with a transcript. Each legal representative who refused conducting intradermal tests for tuberculosis infection, it is mandatory to be invited to a meeting of the medical commission of a medical organization (Order of the Ministry of Health and Social Development of Russia dated May 5, 2012 No. 502n “On approval of the procedure for the creation and activities of a medical commission of a medical organization”). At the same time, additional information is provided about the recommended medical intervention and the consequences of refusing it. The reasons for the refusal are being clarified.
If the parents (legal representatives) of the child refuse intradermal tests (Mantoux, ATP), it is possible to prescribe alternative examination methods in order to exclude tuberculosis in the child.
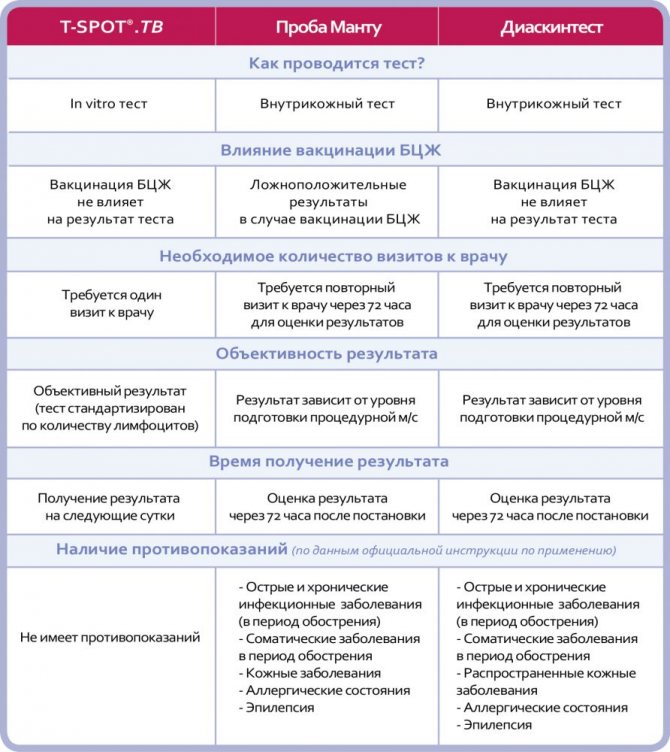
Alternative methods for testing for tuberculosis infection include in vitro diagnostic tests. There are currently two commercial diagnostic tests based on this technology. One of them is QuantiFERON®-TB Gold, the other test is T-SPOT.TB (registered in Russia). A negative result of in vitro tests (T-SPOT.TB) in the absence of clinical symptoms of the disease (respiratory and intoxicating nature, other local pathological manifestations) allows the TB doctor to issue a certificate stating that the child does not currently have active tuberculosis.
If you refuse immunodiagnostics (any other method that allows you to exclude tuberculosis), the TB doctor determines the possibility of issuing a certificate or medical report about the absence of an active form of tuberculosis. Deciding on the admission of a child to an educational organization is not within the competence of a TB doctor.
The grounds for a TB doctor to issue a certificate or medical report are:
— results of screening examination for tuberculosis;
— results of alternative examination methods;
- results of a fluorographic examination of the child’s environment no more than 6 months old;
— data from radiation methods for examining the chest organs;
— data on contact with tuberculosis patients;
- the absence or presence of complaints or symptoms in the child that are suspicious of tuberculosis.
Carrying out preventive chemotherapy for LTBI reduces the risk of developing tuberculosis in the future by 5-7 times.
Indications for preventive chemotherapy:
• positive reactions to recombinant tuberculosis allergen;
• positive reactions to in vitro tests;
· presence of contact with tuberculosis patients;
· high risk of developing tuberculosis (HIV infection, treatment with drugs that cause immunosuppression, etc.).
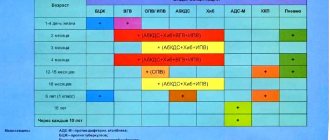
In order to prevent tuberculosis in children, it is recommended to carry out a set of measures to help prevent MBT infection and the emergence of new cases of tuberculosis. The most effective measure is to prevent contact with a patient with an active form of tuberculosis, as well as vaccination against tuberculosis in accordance with the National Preventive Vaccination Calendar. Anti-tuberculosis vaccination prevents severe common forms of the disease in children, reducing the risk of death.
Artanova Marina Vladimirovna, phthisiatrician of the Khanty-Mansi Autonomous Okrug-Yugra “Nyagan City Children's Clinic”
Replacement of Mantoux - Diaskintest: what is it, what will show the result better
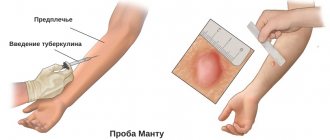
Diaskintest also applies to tuberculin diagnostics, like the Mantoux test, therefore it is considered the best replacement. Using a syringe with a thin needle, only 1 dose of purified tuberculin is injected into the skin. The result is assessed after 72 hours. The specificity of the test is much higher, since tuberculin is administered without protein impurities that cause allergic reactions.
An important feature: this method helps determine whether increased sensitivity is a manifestation of mycobacterial infection or a routine vaccination. Therefore, it can be prescribed if Mantoux results are questionable.
Diaskintest allows you to most objectively conduct a study for patients with reduced immune defense, diabetes mellitus, taking hormones and other drugs to suppress the immune system.
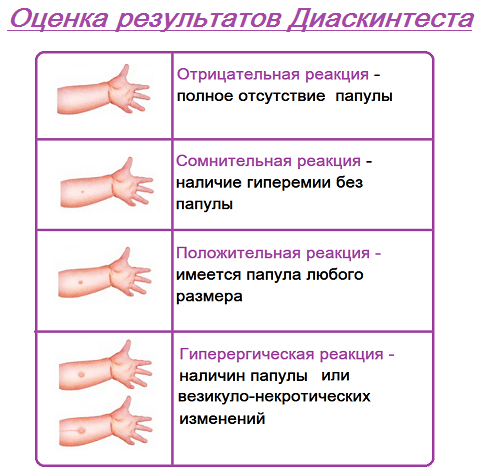
Like the Mantoux test, this skin test is suitable for assessing therapy (preventive or specific anti-tuberculosis). No diagnosis is made based on Diaskintest data. If a questionable or positive result is obtained, an additional examination is prescribed (examination by a phthisiatrician, radiography, sputum culture).
Diaskintest causes allergic reactions much less frequently than the Mantoux test, but they are not completely excluded. There may be a skin rash, itching, bronchospasm, swelling of the skin, and in severe cases, shock. For 1-2 days after the test, there may be a slight increase in temperature, headache, and general weakness.
Watch this video about the benefits of Diaskintest and in what cases it is performed:
Sample analogue - PCR for kindergarten
PCR is a polymerase chain reaction that helps to find the DNA of the tuberculosis bacillus in the blood; it is suitable for kindergarten as an analogue of the Mantoux test. Its disadvantage is the difficulty of finding a laboratory where individual strains can be identified after a vaccine or during infection.
This method is highly sensitive, but at an early stage after the penetration of mycobacteria, their number is extremely low; they penetrate into lymphocytes and do not circulate in the blood. Therefore, PCR is not suitable for determining the risk of tuberculosis, but only detects the developed disease.
Method of collecting blood for tuberculosis in children
For children, blood is taken from a vein to test for tuberculosis. This does not require special preparation, but the day before it is better to avoid overeating and eating too fatty foods. The last meal is taken 8 hours before the visit to the treatment room. In the morning you can only drink water, and you need to have breakfast after drawing blood.

To take material for PCR, special consumables are required - sterile disposable containers with anti-clotting solutions, vacuum systems. It is important to deliver the sample to the laboratory as soon as possible; in exceptional cases, the test tubes are stored at a temperature of 4-8 degrees.
Result evaluation
A qualitative PCR test for tuberculosis gives two types of results - positive or negative. This means the presence or absence of mycobacteria. When quantitatively determined, the tubercle bacilli are reflected in the analysis as concentration (IU/ml). This helps to establish the activity of the infectious process.
An alternative to Diaskintest and Mantoux - quantiferon test
As an alternative for skin tests (Diaskintest and Mantoux), quantiferon can be chosen. It is suitable for selecting patients (screening) who need further examination.
To whom is it assigned?
Indications:
- negative Mantoux or Diaskintest in children with HIV infection, diabetes mellitus, malnutrition, blood tumors;
- contraindications to the administration of tuberculin - intolerance, allergies, skin diseases, infections or recent vaccination, epilepsy;
- questionable skin test result;
- the need to distinguish between positive Mantoux after vaccination and due to infection;
- examination of patients of special social groups (they may not come at the right time to assess the Mantoux results) or those who were in contact with patients;
- confirmation of tuberculosis by symptoms (cough, bloody sputum, fever), positive skin tests, changes in the lungs on an x-ray.
Advantages
The Quantiferon test has the following advantages:
- high percentage of reliable results, no false results after BCG vaccination;
- sufficient specificity and sensitivity;
- safe;
- no adverse reactions or contraindications;
- Just one visit to the doctor is enough;
- subjective assessment is excluded (for example, incorrect measurement of the papule).
Methodology for conducting the quantiferon test
Flaws
Even this modern diagnostic method has disadvantages:
- false results in a child under 5 years of age;
- does not show infection with reduced immunity;
- not suitable for detecting early stage tuberculosis;
- it is impossible to distinguish an active disease from a harmless carriage;
- a negative result is not a 100% guarantee of the absence of tuberculosis;
- Errors in blood collection and transportation may affect reliability.
Watch this video about the advantages and disadvantages of the quantiferon test:
Detailed description of the study
Tuberculosis (TB, Tb) is a chronic infectious disease caused by Mycobacterium tuberculosis (Mycobacterium tuberculosis, MBT). MTB can affect all organs and tissues, but most often tuberculosis infection affects the lungs. Tuberculosis can affect both adults and children.
The difficulty of diagnosing tuberculosis is based on the various variants of the course of the infection. There are active tuberculosis (with clinical manifestations) and latent, or latent, tuberculosis infection (LTBI). LTBI is characterized by the presence of Mycobacterium tuberculosis in the body, which can be detected using special laboratory tests, but the presence of MBT in the body is not accompanied by clinical and radiological signs of TB infection.
The goal of LTBI detection is to prevent progression of asymptomatic TB infection to active TB and to initiate treatment early. The most common method for detecting LTBI is the tuberculin skin test (TST) or Mantoux test. Thanks to this test, MTB infection is determined, risk groups for TB infection are formed, and individuals are selected for vaccination or revaccination against tuberculosis. This test is also used to diagnose TB in children. However, the Mantoux test has a number of disadvantages, which include:
- Subjectivity when interpreting results;
- Lack of differentiation between active TB and LTBI;
- Insufficient diagnostic sensitivity in immunocompromised patients;
- The likelihood of false-positive results in patients who have been vaccinated with BCG (tuberculosis vaccine) or infected with mycobacteria that do not cause TB.
In this regard, an alternative diagnostic method was developed - QuantiFERON-TBtest (QFT), or quantiferon test. It is based on the determination of specific proteins in the blood - gamma interferons (γ-IFN), which are produced by T-lymphocytes in response to the entry of mycobacterium tuberculosis into the body. The advantages of QFT include:
- High specificity and sensitivity compared to TST;
- The result does not depend on previous BCG vaccination;
- Safety: unlike the Mantoux reaction, the study does not involve the introduction of any substances into the body.
This method, as an alternative to the Mantoux test, is approved by many authoritative medical societies, including the World Health Organization.
However, like the Mantoux test, the quantiferon test does not distinguish active tuberculosis from latent tuberculosis infection, so the result of this analysis must be compared with the clinical picture of the disease, X-ray diagnostic data and other studies.
T-spot test for tuberculosis instead of Mantoux in a child
Instead of Mantoux, a T-spot blood test is performed on the child; it is indicated for detecting active and latent tuberculosis infection. It can be the main or auxiliary method, in combination with tuberculin tests it gives the most reliable result.
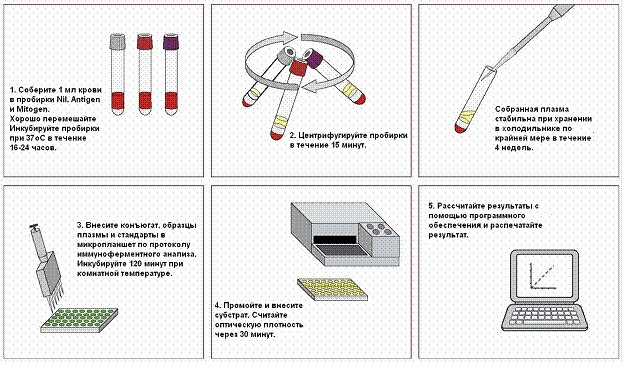
The analysis is carried out on venous blood and consists of counting T-lymphocytes that have been in contact with Mycobacterium tuberculosis. The main advantages and disadvantages are similar to the quantiferon test.
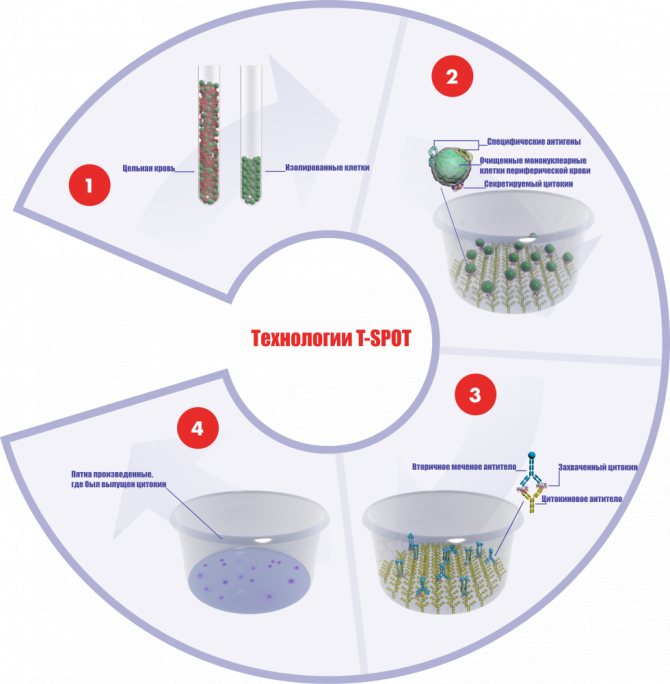
Scheme of T-spot analysis for tuberculosis
X-ray for diagnosis
X-rays can be performed on a child of any age. It is used to diagnose tuberculosis only when indicated - changes in the blood or positive skin tests. Prescribed by a pediatrician or phthisiatrician. Infants need the presence of an adult, as complete stillness is required during photographs.
The risk of the procedure is associated with X-ray exposure, so you can undergo no more than one examination per year. However, if there is a threat of pulmonary tuberculosis, a repeat study is possible. This method will most accurately indicate the presence of a pulmonary form of infection, but it will not help in any way with the latent form of the disease.

Which test is best for children?
For children, skin testing is best. Contrary to the prevailing opinion about their danger, the intake of allergen into the body is minimal, and only they show the latent phase of tuberculosis.
Diaskintest currently gives the best results, it is less dangerous with the risk of intolerance. However, not all mycobacteria can be detected by neem. Therefore, the Mantoux test remains relevant for the initial selection of children who are indicated for an in-depth examination.
Blood tests are expensive, no higher in reliability than Mantoux and Diaskintest, but the most important thing is that they will not show differences in active tuberculosis and carriage of mycobacteria. Since the second group in the world is approaching 1.7 billion, and only 10 million of them are sick, this difference is significant.
We recommend reading about how many days after Mantoux is checked. From the article you will learn on what day Mantoux is tested in a child, when it is done, the reactions of the Mantoux test and how to check the result yourself. And here is more information about what you can’t eat with Mantoux.
An alternative to Mantoux for children is a safer skin test with tuberculin - Diaskintest. In case of intolerance, blood tests are prescribed - PCR, quantiferon test and T-spot. To clarify the diagnosis, a chest x-ray is performed.
Mantoux or safe diagnosis of a child for tuberculosis – what do parents have the right to choose?
The issue of removing children without Mantoux from kindergarten or school is becoming increasingly acute - parents do not want to give their children potentially dangerous and uninformative diagnostics, and for this their children are not allowed into educational organizations.
How can such a situation be assessed from the point of view of the law and what should parents do?
So there is a problem:
Schools and kindergartens are suspended from attending children who have not received Mantoux or if they have not provided a certificate from a TB doctor. A TB doctor can examine the child and issue the necessary certificate, but...
But in practice, the TB doctor does not issue a certificate if the child has not done an x-ray or a Diaskin test. However, X-rays, Diaskin test, and Mantoux are all unsafe diagnostic methods. Moreover, the information content of these examination methods is poor.
Relatively speaking, even if the child undergoes all these examinations and the result is negative, it is impossible to say that he is healthy, because for the same Mantoux reaction the indicator is 50-60 percent.
But you can just as well guess about a child who refuses to undergo this examination - he can also be healthy or unhealthy.
Understanding this, many parents do not want to conduct unsafe examinations again. And they do have the right to refuse medical intervention. And why all these examinations, if the child is outwardly healthy, there are no signs of disease? – parents reason in this way.
But there are SanNiPs, where it is established that in order to attend an educational institution, a child must provide either Mantoux results or a phthisiatrician’s conclusion.
It is important that this is stated precisely in SanPiNs, and not in federal law. But this does not make it any easier for parents - if previously cases of children being excluded from attending educational organizations were rare, and the prosecutor’s office sided with parents and children, and even the Commissioner for Children’s Rights Pavel Astakhov was forced to intervene to protect the rights of the child, now the situation has changed. Federal legislation has not changed, but its interpretation by the same prosecutor's office has changed.
Does this mean that the right to education now depends on the availability of vaccinations and Mantoux?
It is premature to draw conclusions. Parents who have made a tough decision not to give their child Mantoux should understand that there is a court that can consider the dispute.
But all these requirements of the Ministry of Health for the prevention of tuberculosis did not arise out of nowhere - the safety of children in educational organizations must be ensured, the only question is in what way, at what cost.
Is there an alternative to Mantoux and X-ray when diagnosing tuberculosis?
There are alternatives - the quantiferon test and the T-SPOT test.
Both of these tests, unlike Mantoux, are done for a fee.
T-SPOT results are accepted by doctors to give an opinion, and the child will be able to attend kindergarten and school.
T-SPOT has higher sensitivity (92%) and specificity (97%) than the 2-TE Mantoux test. It is especially important that the test results are not affected by BCG vaccination in childhood. This test is at least 6 times more accurate than the skin test in predicting the development of active tuberculosis.
It is important that T-SPOT is carried out in vitro – i.e. nothing is injected into the child’s body; on the contrary, blood is drawn, which is examined, and after 3 days you can receive the test results.
T-SPOT has been registered and used in Russia since 2012 (registration certificate No. FSZ 2012/648).
So why don't children get T-SPOT for free instead of Mantoux, if using T-SPOT is preferable?
It's all about the cost - performing a Mantoux test on a child costs about 500-550 rubles, and T-SPOT costs about 6 thousand rubles.
Of course, conducting such an expensive examination on all children is not an option for the compulsory medical insurance fund. Therefore, the majority are examined using the Mantoux reaction - it’s cheap, suitable for show in terms of carrying out anti-tuberculosis measures, but the information content is low, and safety is lame (by the way, the pesticides included in the Mantoux reagent (phenol, Tween-80) have toxic properties and can cause negative consequences for the child).
But what about the law - does it allow for diagnostics that have contraindications and a lot of adverse reactions?
The law does not prohibit this, but another thing is that you must give consent to this.
Those. a person must understand what is involved in medical intervention. That is why parents have the right not to give their child vaccinations, or the Mantoux test, or x-rays (Diaskin test). All this is voluntary. But now it turns out that if this is not done, the child is not allowed to go to school or kindergarten. And this already turns out to be a kind of coercion. While the basic law of the country does not provide for this.
What does the law say on education and medicine?
The right to health protection is guaranteed to everyone by the Constitution of Russia - Article 41 clearly states this right, as well as the fact that concealment by officials of facts and circumstances that pose a threat to the life and health of people entails liability in accordance with federal law .
The right to education is established in Article 43 of the Russian Constitution. Universal access and free preschool, basic general and secondary vocational education in state or municipal educational institutions and enterprises are guaranteed.
And not a single article of the Constitution or any other federal law says that a child can receive education provided that he has all the vaccinations and has been diagnosed for tuberculosis using the Mantoux test or X-ray.
The Constitution does not set any conditions for receiving education. Moreover, a child can receive education in different forms - incl. at home instead of going to school every day. But it is the parent who has the right to decide exactly how to educate their child.
So what's the problem?
But the problem is that now in the era of the global Internet, absolutely any information is publicly available. Therefore, if previously ordinary people generally could not read instructions for medications, scientific articles by many authors (including foreign ones), now this can be easily done. Therefore, many parents have become more literate in these matters and do not want their child to undergo unsafe examinations just like that without indicating that the child may have a disease. At the same time, they agree to conduct safe examinations - for example, T-SPOT.
But not everyone has the money for this. The problem is that Mantu can be made for free, but T-SPOT cannot.
But at the same time, as it became known, the results of T-SPOT are accepted instead of Mantoux; in this case, phthisiatricians without any problems issue the necessary certificates for a school or kindergarten - of course: after all, unlike Mantoux, this test is almost 100% reliable.
But what to do if there is no money to pay for safe diagnosis of tuberculosis - every year not every parent is ready to shell out 6 thousand rubles from their pocket so that the child is not suspended from school or kindergarten. And this despite the fact that regarding other children who received Mantoux, there is still uncertainty - whether they are healthy, because... Mantoux information content is 50-60%.
There are options for action:
1. Agree and give the child Mantu.
2. Refuse Mantoux and demand in writing that the medical institution provide the opportunity to conduct a safe examination for tuberculosis, for example, through T-SPOT. If they refuse, complain to the prosecutor's office, the Ministry of Health, the Commissioner for Children's Rights, etc. – this is the case if the child is also deprived of the right to education. You can even go to court.
3. Refuse Mantoux and request in writing that the medical institution (TB doctor) issue a conclusion based on the data from the child’s examination and other safe tests, incl. taking into account the fact that family members living with the child are not registered with the TB doctor. If it doesn’t work, complain as indicated in point 2.
4. Pay for the T-SPOT analysis for the child yourself and demand that these results be accepted and the child not be prevented from attending educational institutions. Usually, in this case, no problems arise (parents, for example, from the Tula region report this).
And one more important point - if this issue of alternative safe examinations had been regulated by federal law, then no SanPiNs would have stood in the way of a child without Mantoux who wanted to attend school or kindergarten.
To do this, it is necessary to stipulate at the legislative level, for example, when parents can choose a more expensive diagnostic method and have it carried out at the expense of the compulsory medical insurance fund, rather than paying for it out of their own pocket.
Can each parent individually influence this?
Yes maybe.
0
Author of the publication
offline for 3 days
GarryB83
0
Comments: 0Publications: 1256Registration: 07/17/2018