Pharmacological properties of the drug Cytoflavin
A metabolic agent, the pharmacological effects of which are due to the complex effects of the components of the drug. Stimulates respiration and energy production in cells, improves the processes of oxygen utilization by tissues, restores the activity of antioxidant enzymes. The drug activates intracellular protein synthesis, promotes the utilization of glucose, fatty acids and resynthesis of GABA in neurons through the Roberts shunt. Cytoflavin improves coronary and cerebral blood flow, activates metabolic processes in the central nervous system, restores consciousness and intellectual-mnestic functions of the brain, eliminates reflex disorders and sensitivity disorders. It has a quick awakening effect during post-anesthesia depression of consciousness. When using Cytoflavin in the first 12 hours from the onset of stroke, a favorable course of ischemic and necrotic processes in the affected area (reduction of the lesion), restoration of neurological status and a decrease in the level of disability in the long-term period are noted. It has a positive effect on the parameters of neurological status: it reduces the severity of asthenic, cephalgic, vestibulo-cerebellar, cochleovestibular syndrome, and also eliminates disorders in the emotional-volitional sphere (reduces the level of anxiety, depression). Improves cognitive-mnestic functions and improves quality of life. With intravenous infusion at a rate of about 2 ml/min (in terms of undiluted Cytoflavin), succinic acid and riboxin (inosine) are utilized almost instantly and are not detected in the blood plasma. Riboxin (inosine) is metabolized in the liver to form glucuronic acid and its subsequent oxidation. A small amount is excreted by the kidneys. Nicotinamide is rapidly distributed in all tissues, penetrates the placenta and into breast milk, is metabolized in the liver to form nicotinamide-N-methylnicotinamide, and is excreted by the kidneys. The half-life from blood plasma is about 1.3 hours, the volume of distribution at steady state is about 60 l, and the total clearance is about 0.6 l/min. Riboflavin: distribution is uneven - the largest amount accumulates in the myocardium, liver, and kidneys. The half-life from blood plasma is about 2 hours, the volume of distribution at steady state is about 40 l, and the total clearance is about 0.3 l/min. Penetrates through the placenta and into breast milk. The degree of binding to blood proteins is 60%. Excreted by the kidneys, partly in the form of a metabolite; when administered in high doses - mainly unchanged.
pharmachologic effect
Metabolic drug. Pharmacological effects are due to the complex effect of the components included in the drug Cytoflavin ®. Stimulates the processes of cellular respiration and energy formation, improves the processes of oxygen utilization by tissues, restores the activity of enzymes that provide antioxidant effects.
The drug activates intracellular protein synthesis, promotes the utilization of glucose, fatty acids and the resynthesis of GABA in neurons through the Roberts shunt.
Has a positive effect on the bioelectrical activity of the brain.
Cytoflavin ® improves cerebral and coronary blood flow, activates metabolic processes in the central nervous system, reduces reflex disorders, helps restore impaired sensitivity and intellectual-mnestic functions of the brain.
It has a positive effect on the parameters of neurological status: it reduces the severity of asthenic, cephalgic, vestibulo-cerebellar, cochleovestibular syndrome, and also eliminates disorders in the emotional-volitional sphere (reduces the level of anxiety, depression). Improves cognitive-mnestic functions and quality of life.
When administered intravenously, it helps restore impaired consciousness. It has a quick awakening effect during post-anesthesia depression of consciousness. When using Cytoflavin in the first 12 hours from the onset of stroke, a favorable course of ischemic and necrotic processes in the affected area (reduction of the lesion), restoration of neurological status and a decrease in the level of disability in the long-term period are observed.
Use of the drug Cytoflavin
Only IV drip diluted in 100–200 ml of 5–10% glucose solution or 0.9% sodium chloride solution. In case of acute cerebrovascular accident, the drug is administered as early as possible from the onset of the disease in a volume of 10 ml per injection with an interval of 8–12 hours for 10 days. In severe cases of the disease, the single dose is increased to 20 ml. For discirculatory encephalopathy and the consequences of cerebrovascular accidents, the drug is used in a volume of 10 ml once a day for 10 days. For toxic and hypoxic encephalopathy, the drug is administered in a volume of 10 ml per injection 2 times a day with an interval of 8–12 hours for 5 days. In case of coma, administer in a volume of 20 ml per 200 ml of glucose solution. For post-anesthesia depression, it is administered once in the same doses. Cytoflavin tablets are taken orally, 2 tablets 2 times a day, 30 minutes before meals, without chewing, at intervals of 8–10 hours, with 100 ml of water. Course duration: 25 days (100 tablets per course). Evening administration of the drug is recommended no later than 18:00. A repeat course is prescribed when the manifestations of cerebrovascular insufficiency increase, but not earlier than 25–30 days after the end of the previous course.
Indications for use
In adults in complex therapy:
– cerebral infarction; – consequences of cerebrovascular diseases (cerebral infarction, cerebral atherosclerosis); – toxic and hypoxic encephalopathy in acute and chronic poisoning, endotoxicosis, post-anesthesia depression of consciousness, as well as for the prevention and treatment of hypoxic encephalopathy during cardiac surgery using artificial circulation, for the prevention of cognitive disorders after extensive surgical interventions in elderly patients.
In children
In children (including premature infants with a gestation period of 28–36 weeks) in complex therapy in the neonatal period: – with cerebral ischemia.
Side effects of the drug Cytoflavin
With rapid intravenous drip administration, undesirable reactions may occur that do not require discontinuation of the drug: hyperemia of the skin of varying severity, a feeling of heat, bitterness and dry mouth, sore throat. With long-term use in high doses, transient hypoglycemia, hyperuricemia, and exacerbation of gout are possible. Rare adverse reactions include short-term pain and discomfort in the epigastric region and chest area, difficulty breathing, nausea, headache, dizziness, “tingling” in the nose, dysosmia, pallor of the skin of varying severity. Allergic reactions such as itchy skin are also possible.
Side effect
According to the World Health Organization, adverse effects are classified according to their frequency as follows:
– very frequent (≥ 1/10); – common (≥ 1/100 – – uncommon (≥ 1/1000 – – rare (≥ 1/10000 – – very rare ( – frequency unknown (cannot be determined from available data). Immune system disorders: very rare - hypersensitivity reactions, anaphylactic shock. Nervous system disorders: very rare - headache, dizziness, paresthesia, tremor, hypoesthesia. Mental disorders: very rare - psychomotor agitation (restlessness, increased motor activity). Cardiac disorders: very rare. - tachycardia, short-term pain and discomfort in the chest, a feeling of increased or increased heart rate. Vascular disorders: very rarely - increased or decreased blood pressure, hyperemia or pallor of the skin of varying severity. Disorders of the respiratory system, thoracic organs cells and mediastinum: very rarely - difficulty breathing (shortness of breath), suffocation, sore throat, dry cough, hoarseness, nasal paresthesia, dysosmia, bronchospasm. Gastrointestinal disorders: very rarely - bitterness, dryness, metallic taste in the mouth, short-term pain and discomfort in the epigastric region, nausea, vomiting, oral hypoesthesia, dyspepsia. Disorders of the skin and subcutaneous tissues: very rarely - itching, rash, swelling of the face, urticaria, angioedema, sweating. Metabolic and nutritional disorders: very rarely - transient hypoglycemia, hyperuricemia, exacerbation of gout. Children (including premature babies) may develop alkalosis during the neonatal period. General disorders and disorders at the injection site: rarely - chills, feeling hot, weakness, increased body temperature, pain and redness along the vein. Laboratory and instrumental data: very rarely - rapid breathing. To avoid unwanted reactions, it is recommended to follow the dosage regimen and rate of administration of the drug. If any of the adverse reactions indicated in the instructions worsen or you notice any other adverse reactions not listed in the instructions, notify your doctor.
Special instructions for the use of the drug Cytoflavin
Use with caution for nephrolithiasis, gout, hyperuricemia. Can be used during pregnancy (in the absence of allergic reactions to the components of the drug). In critical conditions, the drug should be used after normalization of central hemodynamic parameters. It is possible that blood glucose levels may decrease (which must be taken into account when prescribing), and urine may turn light yellow. In case of hypertension (arterial hypertension), dose adjustment of antihypertensive drugs may be required.
special instructions
When taking Cytoflavin orally, dose adjustment of antihypertensive drugs may be required in patients with arterial hypertension.
In critical conditions, intravenous administration of the drug is possible after normalization of central hemodynamic parameters.
During treatment, blood plasma glucose levels should be monitored.
During the administration of the drug, urine may turn light yellow.
Impact on the ability to drive vehicles and operate machinery
When taken orally, the drug does not affect the ability to concentrate.
Drug interactions Cytoflavin
succinic acid, inosine, nicotinamide are compatible with other drugs. Riboflavin: reduces the activity of doxycycline, tetracycline, oxytetracycline, erythromycin and lincomycin. Incompatible with streptomycin. Chlorpromazine, imizine, amitriptyline, by blocking flavin kinase, disrupt the incorporation of riboflavin into flavin adenine mononucleotide and flavin adenine dinucleotide and increase its excretion in the urine. Thyroid hormones accelerate the metabolism of riboflavin. Reduces the severity and prevents the side effects of chloramphenicol (disturbance of hematopoiesis, optic neuritis). Compatible with drugs that stimulate hematopoiesis, antihypoxants, and anabolic steroids.
Experience with the use of cytoflavin in very premature infants
Key words : very premature newborns, post-hypoxic myocardial damage, post-hypoxic damage to the central nervous system, intraventricular hemorrhage, acid-base state, lactate, cytoflavin.
To reduce the damaging action of hypoxia and to correct severe metabolic and cardiac disorders in critically ill premature newborn infants, metabolic therapy with cytoflavin was studied in extremely premature infants (33 and 25 babies in a study group and a comparison one, respectively). The use of this drug in extremely low and very low birthweight babies with posthypoxic myocardial damage and severe metabolic disorders was found to lead to normalization of acid-base balance within 24 hours after treatment initiation. During the therapy, there was a marked cardiocytoprotective effect and no increase in the degree of intragastric bleedings.
Key words : extremely premature newborn infants, posthypoxic myocardial damage, posthypoxic CNS damage, intragastric bleedings, acid-base balance, lactate, cytoflavin.
Among the etiological factors that are most significant in the pathogenesis of perinatal cerebral damage in newborns, the main role belongs to hypoxia 1. Fetal hypoxia develops as a result of the pathological course of pregnancy and leads to the birth of a premature baby with respiratory disorders. Very premature newborns have a number of anatomical and physiological features, such as hypercatecholaminemia, loose type of coronary arteries and physiological carnitine deficiency. The consequence is a sharp decrease in the formation of macroergs in the mitochondria of cardiomyocytes, the predominance of the carbohydrate component of metabolism and the launch of a cascade of disorders. As a result of hypoxia, respiratory acidosis is formed, tissue hypoxia and metabolic acidosis develop secondarily in the tissues.
Hypercatecholaminemia initially has a stimulating effect on the vasomotor center, increased cardiac activity, increased arteriolar tone and a tendency to hypertension are noted. Arrhythmia gradually appears, the sensitivity of adrenal receptors to catecholamines decreases, and heart failure increases. A very premature newborn becomes unable to adequately survive the massive restructuring of the blood circulation, which leads to high functional tension of the cardiovascular system and the opening of fetal communications; as a result of the addition of metabolic acidosis, circulatory disorders in all tissues are aggravated, cerebral circulatory disorders occur and, as a consequence, an unfavorable neurological outcome.
This led to the search for a method to reduce the damaging effects of hypoxia and the severity of critical condition in premature newborns requiring resuscitation and intensive care.
The use of a number of metabolic drugs introduced into neonatology from adult practice (Mexidol, Instenon, etc.) and vital in intensive care situations has limitations when used in newborns due to the drug being prescribed not in full accordance with the instructions. In 2004–2009 under the leadership of academician RAMS prof. N.N. Volodin, a multicenter, double-blind, randomized study of the parenteral form of the drug Cytoflavin (Scientific and Technological Pharmaceutical LLC, St. Petersburg, Russia) was conducted in premature newborns with hypoxic-ischemic damage to the central nervous system of varying severity 2. In this regard, it seems important to supplement these studies with a study of the condition cardiovascular system against the background of metabolic therapy with cytoflavin.
Purpose of the study: To analyze new approaches to metabolic therapy in very premature infants in the neonatal intensive care unit.
Characteristics of children and research methods The study was conducted at the Presidential Perinatal Center of the Ministry of Health and Social Development of Chuvashia. In order to correct severe metabolic and cardiac disorders, cytoflavin was used intravenously at a dose of 2 mg/kg per day after dilution in a 10% glucose solution in a ratio of 1:5. The drug was administered for 5 days, according to the recommendations for the treatment of premature CO by Rogatkin (2012). The rate of administration of the resulting solution ranged from 1 to 4 ml/h.
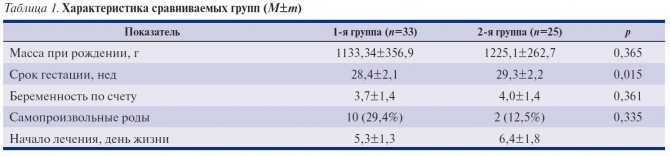
The drug contains sodium succinate, inosine, riboflavin and nicotinamide 3. To study the clinical effectiveness of cytoflavin for the prevention and treatment of hypoxic brain damage, myocardial ischemia and correction of metabolic disorders in premature infants, we identified groups of premature infants with long-term (more than 48 hours) metabolic disorders according to the acid-base state (ABC). In children of the 1st group (main group, 33 children), cytoflavin was administered against the background of basic intensive therapy (permission of the ethical committee at the Chuvash State University named after I.N. Ulyanov No. 8 dated March 01, 2013), in 2 The 2nd group (comparison group, 25 children) received only basic intensive therapy. The characteristics of the compared groups are presented in the table.
The dynamics of acid-base balance indicators, electrocardiography (ECG), echocardiography (Echo-CG), and neurological status were analyzed. Functional research methods were carried out in the department of functional diagnostics. Echocardiography was performed on children on days 1, 2–4, 5–7 of life using an ALOKA1700, LOGIQ book XP device with microconvex sensors with a scanning frequency of 5 MHz. Standard ECG examination - on days 1–2, 10 of life, then according to indications using the HeartMirror3-IKO device from INNOMED (Japan). Neurosonography was carried out on days 1, 2–4, 5–7 of life.
The work used statistical analysis methods generally accepted in medical research, parametric and nonparametric methods. The reliability of differences was assessed using Student's tests, z-score with Yates' correction, the closeness of connections between characteristics was determined using Spearman correlation analysis. The results obtained were entered into an IBM personal computer database and processed using the licensed statistical software package “Statistika 6.0” in a Windows environment.
Results and discussion
It was revealed that in patients of the main group during therapy from the first hours of treatment there was a rapid normalization of acid-base balance indicators due to the elimination of the metabolic component of mixed acidosis (–6.0±0.3 to –3.1±0.1 mmol/l in 1- group and –5.7±0.2 to –5.0±0.2 mmol/l in group 2). 6–12 hours after the start of treatment, the value of base deficiency (BE) in the group of children receiving metabolic therapy was significantly lower compared to that in the comparison group (–4.7±0.2 mmol/l versus –5.5± 0.2 mmol/l; p=0.001); subsequently, by the end of the 2nd day of life, the indicators remained within normal values until the end of the 5-day course of therapy (–1.4±0.2 mmol/l versus –3.3±0.1 mmol/l in the comparison group ; p=0.001).
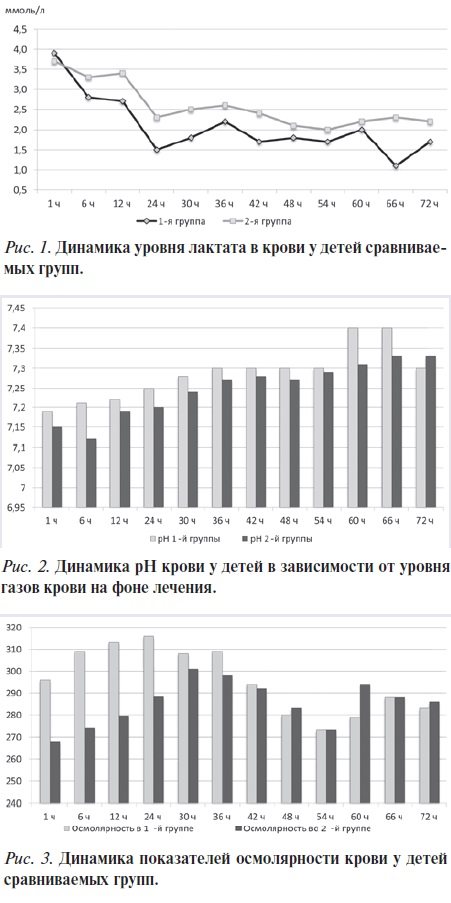
In addition to the BE indicator, we analyzed the dynamics of serum lactate content in children of the compared groups (Fig. 1). The initial lactate level was 3.9±0.2 mmol/l in the 1st group of patients and 3.7±0.2 mmol/l in the 2nd group. After 24 hours, the lactate level in children of group 1 did not exceed normal values (1.5±0.2 mmol/l); in the comparison group it was 2.3±0.1 mmol/l (p=0.001). The dynamics of blood pH indicators is presented in a similar way (Fig. 2). If in the group of children receiving cytoflavin therapy, pH parameters close to normal values (pH7.28) were obtained already at the beginning of the 2nd day from the start of therapy, then in the comparison group this parameter was achieved at the end of the 2nd day from the start therapy (p=0.043). The dynamics of osmolarity indicators in children of the compared groups is presented in Fig. 3.
During the first hours of treatment, the O2 concentration in the respiratory mixture in newborns of the main group was reduced to 32%, and then to 25%. Thus, by the end of the 1st day from the start of therapy, the children of the main group received a respiratory mixture containing non-toxic concentrations of oxygen. In children of the 2nd group, the concentration of O2 in the respiratory mixture was higher at the beginning of therapy (45%), which was dictated by acid-base balance indicators and data from transcutaneous monitoring of SpO2. Despite the fact that they tried to reduce the concentration of O2 in the respiratory mixture in the children of the comparison group, it was possible to achieve safe concentrations in this group only by the end of 2 days.
According to the ECG, it was revealed that on the 1st day of life, all patients had sinus rhythm with an average frequency of 145 per minute, a right gram with an average alpha angle of +95° to +158°, the P–Q interval was 0.08–0 , 10 s, duration of the QRS complex – 0.04–0.06 s Pathological changes in the QRST complex in the form of a low-voltage ECG, reflecting a decrease in myocardial contractility in the ischemic zone, were observed in more than half of the children of groups 1 and 2 ( in 53 and 51%, respectively). A deep pathological Q wave with a duration of more than 0.03 ms and an amplitude of more than ¼ of the R wave in at least two chest leads in premature infants was detected in 11.1% of children in group 1 and in 10% in the comparison group.
From the 3rd day of therapy, according to ECG data, signs of electrical instability of the myocardium, energy deficiency, and changes in repolarization decreased in both groups. However, by the 5th day of therapy, the rate of positive ECG changes in the main group was faster and more pronounced than in the comparison group. With similar ECG data, by the 5th day of therapy, the number of patients with persistent ST depression and elevation in the right and left precordial leads exceeded that in the main group by at least 2 times (39.6 and 13.9%, respectively; p = 0.033 and 19.6 and 4.6%, p=0.1). In 15 (45.5%) children of the 1st group and 4 (16%) children of the 2nd group in the right chest leads, the T wave was positive and isoelectric. In 33.3% of patients in group 1, ischemic T wave inversion decreased, while in group 2 it remained in 80% of cases (p = 0.0001). The T wave in the left precordial leads in the main group was initially positive only in 30% of cases; during treatment with cytoflavin, by the 5th day of therapy it became positive in ¾ of patients, and the number of children with T-wave inversion decreased by 4 times (from 26.6 to 6.66%; p = 0.053).
We analyzed the neurological status of newborns over time. It is known that the most common cerebral lesions in very premature newborns are intraventricular hemorrhages and periventricular leukomalacia.
Intraventricular hemorrhages are more often observed in premature newborns as a consequence of the immaturity of the germinal matrix vessels and pose a serious danger to premature infants, as they are one of the main causes of death and severe psychoneurological disorders in the future. Neurosonography in the observed newborns of the two groups revealed an insignificant difference in the frequency and degree of neurological changes. The incidence of grade 1 intraventricular hemorrhage was similar in both groups (39 and 36%, respectively); grade 2 intraventricular hemorrhages were detected in 21.2 and 27.5% of cases, respectively (z=0.08, p=0.93); Grade 3 hemorrhages were observed 2 times more often in patients in the comparison group, but the difference was not significant (5.8 and 10.1% of patients, respectively, z=0.097, p=0.92). An insignificant difference in the syndrome of central nervous system depression was noted in children of the compared groups on the 5th day of therapy, although this syndrome occurred 2 times less often in group 1 than in group 2 (4.3 and 9.5% of patients, respectively; z = 0.08, p=0.90).
During cytoflavin therapy, there was no increase in the degree of intraventricular hemorrhage, and in patients of group 2 (35.4%) a combination of periventricular leukomalacia and intraventricular hemorrhage was observed against the background of deep brain immaturity. We conducted a correlation analysis between the degree of intraventricular hemorrhage and the therapy performed in the compared groups and did not reveal a significant difference (in group 1 r = +0.12, p = 0.12, in group 2 r = +0.19, p=0.15).
conclusions
Thus, the use of Cytoflavin in children with extremely low and very low body weight with post-hypoxic myocardial damage and severe metabolic disorders leads to the normalization of acid-base balance levels within 24 hours from the start of treatment (p = 0.043), the BE parameter to -3.0 ± 0, 1 mmol/l (p=0.001), lactate level up to 1.5±0.2 mmol/l (p=0.001) and a pronounced cardiocytoprotective effect.
Bibliography
1. Perlman JM Neurology: neonatology questions and controversies. Saunders, Elsevier, 2008; 225. 2. Volodin N.N., Rogatkin S.O., Lyudovskaya E.V. Treatment of children who have suffered perinatal hypoxia during the period of early neonatal adaptation. Vopr Gynecol, Akush and Perinatol 2005; 1:20–25. (Volodin NN, Rogatkin SO, Ljudovskaja EV Treatment of children with perinatal hypoxia during the early neonatal adaptation. Vopr ginekol, akush i perinatol 2005; 1: 20–25.) 3. Rogatkin S.O. Diagnosis, prevention and treatment of perinatal posthypoxic lesions of the central nervous system in newborns and young children a. Author's abstract. dis. ... doc. honey. Sci. M 2012; 44. (Rogatkin SO Diagnosis, prevention and treatment of perinatal posthypoxic lesions of the central nervous system in children and new born his age and injuries. Avtoref. dis. ... dokt. med. nauk. M 2012; 44.)
Source of publication: Russian Bulletin of Perinatology and Pediatrics, 2, 2016Material provided by Polisan LLC