BRIEF HISTORY OF BCG
The first thoughts about the possibility of creating an anti-tuberculosis vaccine came from the French microbiologist Albert Calmette and veterinarian Camille Guérin when they worked at the Pasteur Institute in Lille in 1908.
Scientists have noticed that on a nutrient medium based on glycerin, bile and potatoes, tuberculosis bacilli of the least virulence grow, and, therefore, you can try to grow a culture of weakened tuberculosis microbes. By 1919, scientists had created a strain that did not cause tuberculosis in experimental animals and were thinking about testing it on humans. But it was only on July 18, 1921 that the first BCG vaccinations were given. In the beginning, it often happened that “something went wrong”: for example, in Lübeck, Germany, all of the 240 vaccinated newborns fell ill with tuberculosis, and 77 of them died. But the investigation showed that it was not the BCG vaccine that was to blame, but the negligence of the doctor who stored it in the same container with a culture of classic tuberculosis microbes.
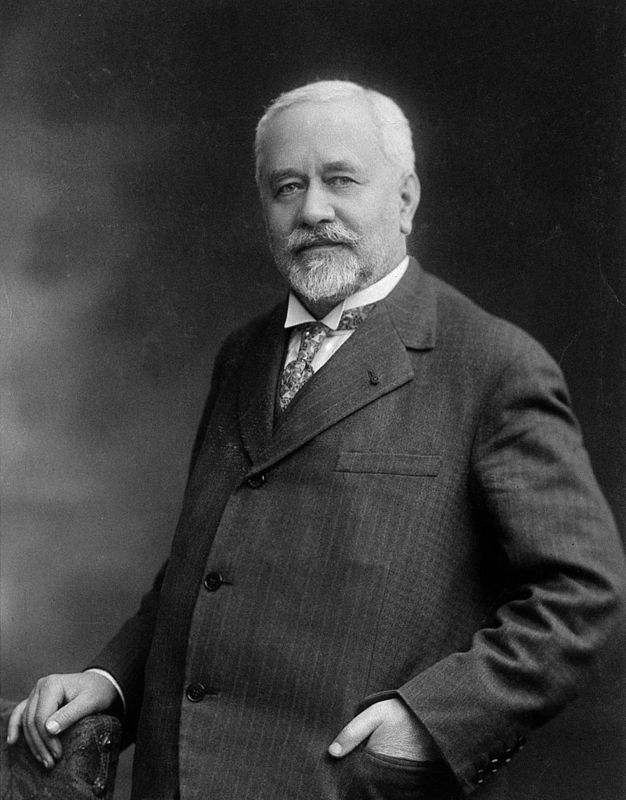
Albert Calmette, 1930
In 1925, Calmette transferred his vaccine to his Soviet colleagues and the BCG vaccination began to be actively used in the USSR. Just 3 years later, it turned out that mortality from tuberculosis in groups of vaccinated children actually decreased. In 1928, it was recommended to vaccinate newborns from “risk groups” with BCG. Since the mid-1950s, vaccination of newborns has become mandatory in most European countries (except perhaps the Netherlands). Also, in 1948, India was the first non-European country to introduce compulsory vaccination; in 1967-1968, Brazil; vaccination is mandatory in Singapore, Malaysia and many other countries. But since the late 1990s, several European countries have stopped using BCG for mass vaccination, citing low incidence of tuberculosis among their citizens.
I will try to simply and briefly talk about the main vaccinations that must be given to a child in the first years of life according to Russian standards. Everything is very simple.
So, first thing. BCG.
1. Every Russian maternity hospital offers two vaccinations: BCG and the first of three vaccinations against hepatitis B.
2. Then, in the first year, according to the national calendar, the baby will have to receive only 1 more vaccination - whooping cough + diphtheria + boletus + polio (it is done three times in 1.5-2 months). Well, repeat the hepatitis B vaccination if it was done in the maternity hospital (it is also done three times).
3. After a year, vaccination against measles + rubella + mumps is given, and then only revaccinations!
BCG is given in the first 3-7 days, in the absence of contraindications, in the shoulder, and if the Mantoux test is negative, revaccination is repeated at 7 and 14 years of age.
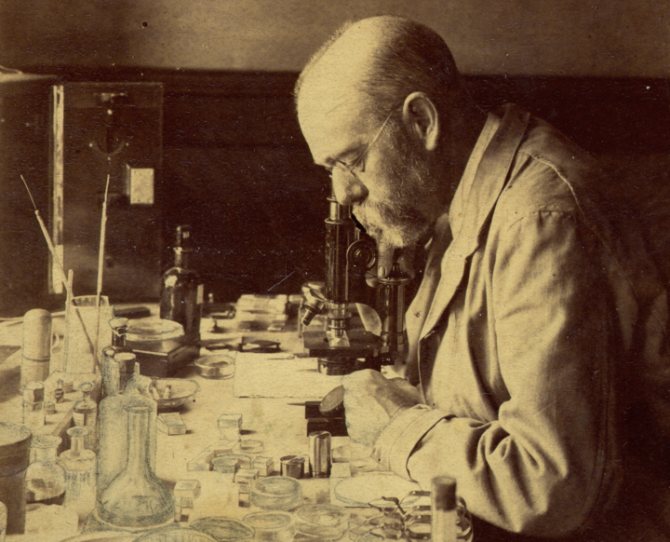
Robert Koch
1. Why do they start with it and how to get infected with it?
They start with BCG because it is believed that there is now a tuberculosis epidemic in our country and there is a very high risk of a newborn baby becoming infected with tuberculosis. It is caused by mycobacteria and is transmitted through the air by sneezing, talking, coughing. Mycobacteria can fly in an elevator, restaurant, airport or subway. In general, the risk of meeting him is high.
Therefore, BCG was traditionally done in the maternity hospital. In addition, it is believed that children more often become ill with tuberculosis during the initial “encounter” with mycobacteria and become more severely ill. In a number of European countries, this vaccination is not carried out because it is believed that the epidemic situation there is favorable (there is currently an ongoing tuberculosis epidemic in Russia).
2. What to do if BCG was not done in the maternity hospital?
Sometimes, for some reason, the child is not given this vaccination in the first days. Then it can be done to the child at your place of residence at any time convenient for you (when you mature, if you are afraid, or when you begin to “go out into the world” with your child). But if you do it after 2 months, you will have to do a Mantoux test first. This is not a vaccination, it is just a test to determine whether the child has already become infected with tuberculosis (in this case, the vaccination is not needed, they will be sent straight to a TB specialist). Sometimes the Mantoux reaction is false-positive, allergic reactions to Mantoux components (to tuberculin) are often observed - then you can do a control so-called Diaskin test, it is more sensitive, and after its result you can decide whether you need to see a phthisiatrician .
3. Complications from vaccination.
BCG is an almost live vaccine, however, the incidence of complications is low even in immunocompromised individuals. Here is what the World Health Organization writes about this: “Complications after BCG vaccination are rare: the incidence of lethal BCG dissemination is estimated at 0.19-1.56 per million vaccinated individuals, and its victims are almost exclusively unintentionally immunized individuals with severe cellular disorders immunity. Significant local reactions, such as extensive local ulceration and regional lymphadenitis, occur in <1:1000 and in the majority of cases (>90%) in immunocompromised individuals. Reports of osteitis have been associated with the use of certain batches of the vaccine, but it is now extremely rare. Because acute adverse events with BCG vaccination are extremely rare, even among HIV-positive infants without clinical signs, all healthy newborns should be vaccinated with BCG, even in HIV-endemic areas.”
4. How does it combine with other vaccinations?
BCG is the only vaccine that is not recommended to be administered together with other vaccines. An interval of approximately 1-1.5 months should be maintained.
Thus, if the vaccination was given to a healthy child in compliance with all the rules for administering the vaccine, it is practically safe, but it greatly reduces the risk of severe forms of tuberculosis in our country, where there is currently an epidemic. If you did not have it done in the maternity hospital, it can be done later, but only after the Mantoux reaction (or Diaskin test) and no earlier than 1 month after/before other vaccinations. The Mantoux test is not a vaccination and is performed after the first year of life every year until adulthood.

Children co-infected with tuberculosis and HIV in Myanmar. © 2012 Matthieu Zellweger (with AIDSpartners.org)
Treatment
To avoid serious complications from an abscess after BCG, treatment should begin at the first signs of its formation.
Several methods are used:
- At the early stage of the formation of a cold abscess, a bandage impregnated with Dimedxide (hormonal ointment) together with Rifampicin is applied to the site of its localization.
- When a size fluctuation of less than 15 mm occurs, the contents of the cold abscess are removed using a syringe. Then a 5% solution of Saluzide or Streptomycin is injected. This operation is performed at intervals of 2 days until complete recovery.
- The ulcer formed after the abscess is treated with a special powder - Isoniazid and covered with a sterile napkin.
Indications for surgery
A surgical operation to remove the abscess and the resulting capsule is performed for a chronic disease.
An abscess whose size exceeds 20 mm is removed in the following ways:
- opened with a scalpel;
- the capsule is excised;
- drainage is carried out.
Then a sterile bandage soaked in an antiseptic solution is applied. It is changed daily.
In addition to the procedures described, a therapeutic course is carried out, which involves the use of anti-tuberculosis drugs.
All identified cases of negative manifestations of vaccination are recorded in the clinic. Children with complications are under constant monitoring in the tuberculosis department. Every 6 months they are examined by a TB specialist.
In addition, they are observed by a pediatrician for 12 months. Any vaccines are strictly prohibited at this time.
“FOR WHITES ONLY?”
When researching the effectiveness of the BCG vaccination, a strange feature was discovered: it “works” effectively only in countries with a temperate climate. Thus, clinical studies conducted in the UK have proven a protective effect of 60% to 80%. But the further south you go, the worse it is, and in countries with an equatorial climate, the effectiveness of BCG turned out to be quite insignificant.
In global statistics, infectious diseases are still the leading cause of death. But in countries with developed healthcare, the average person has already forgotten about the destructive epidemics of the past, and only specialists and lovers of the classics are aware of the horrors of smallpox, cholera or tetanus.
Just a hundred years ago, most children did not live to adulthood, dying from infectious diseases, and only extensive reproduction saved humanity from extinction. Today, in the Russian mortality structure, 1.6% of people die from infections.
While diseases of the cardiovascular system claim the lives of 57% of Russians (according to Rosstat for 2010). Overall life expectancy has increased significantly over the past hundred years, so that in developed countries most people die of “old age” (i.e. cancer, heart attacks and strokes). To what do we owe such happiness? Where did the old epidemics go?

Two women speaking through flu masks during an epidemic, 1918 © Keystone/Getty Images
Sanitary and hygienic measures played a significant role. The incidence of many fecal-oral infections (cholera, typhoid fever, etc.) was minimized when the population began to be supplied with chlorinated water. Outbreaks of the same cholera occur from time to time today, affecting up to 5 million people and killing up to 100 thousand annually, but today this problem concerns almost exclusively 3rd world countries (in 2010, large outbreaks were noted in Nigeria, Chad, Cameroon and Haiti). Only fiction and film classics remind us of past cholera epidemics in Europe (for example, “Death in Venice” by Luchino Visconti).
Antibiotics, which began to be widely used since the 40s of the last century, also played a huge role in the fight against bacterial infections. Wonderful drugs have appeared on the pharmaceutical market that can cure not only bacterial, but also some viral infections, such as viral hepatitis. We will not belittle the importance of condoms in controlling the spread of sexually transmitted diseases.
However, assessing the epidemiological retrospective, we come to the conclusion that vaccines played the greatest role in the fight against dangerous infections. Of course, it is still possible to find an American today with legs paralyzed due to polio, but since the mid-1990s, this disease has no longer been recorded in the Western Hemisphere. There is no longer any smallpox in the world (the last case was registered in Somalia in 1977), but until recently this infection was a planetary disaster.
In the 18th century in Russia, every 7th child died from smallpox, and in the 20th century the virus claimed the lives of almost half a billion people! It was smallpox, as well as other infections brought to South and Central America, that destroyed indigenous civilizations.

Preventive vaccination against cholera in 1966.
The word “vaccine” itself comes from the Latin name for cow (vacca). In 1796, Edward Jenner first used an effective method of preventing smallpox - he inoculated his own son with cowpox, which is non-lethal to humans. Many years before, in the East they began to use rubbing smallpox scabs from people who had had a mild form of smallpox, then the practice of such vaccinations spread to Europe. This is how Jenner himself was vaccinated in childhood. Unfortunately, human smallpox vaccinations were very dangerous and about 2% of children did not survive them. However, smallpox epidemics at that time were so devastating that people preferred such vaccinations as there was less risk. Jenner's ingenious discovery was a successful attempt to inoculate not human, but closely related cowpox. The discovery did not immediately gain fame. Jenner was ridiculed at the Royal Society of London, where he sent his work for evaluation, and was hostile to the idea of inoculating people with cow disease and the clergy. And yet, having gone through a thorny path, vaccination spread throughout Europe during Jenner’s lifetime, and the scientist died in 1823 at the zenith of his fame.
Even during Jenner’s lifetime, vaccination began to acquire the most bizarre myths. Over time, myths changed and new ones replaced outdated ones. However, despite all the resistance to vaccines, smallpox was eradicated by vaccinating almost the entire population of the planet, from civilized Western countries to the illiterate and superstitious natives of Africa. As frightening as the myths about vaccinations sounded, smallpox, which claimed so many lives, was much worse.
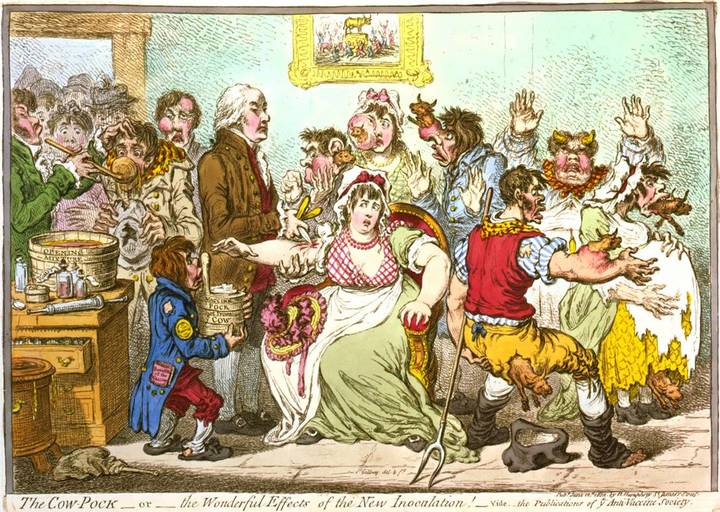
British artist James Gillray in 1802 caricatured the vaccination scene at St. Pancras Hospital. Here Edward Jenner vaccinates frightened girls, while cows jump out of those already vaccinated. At that time, there was a myth that cowpox vaccination could cause the growth of appendages on the body that resembled the body parts of a cow. The boy next to Jenner holds a tub on which is written “Fresh Cow Pocks,” and in his pocket he has a newspaper with the article “Benefits of Vaccine.” The picture at the top of the cartoon depicts the popular biblical scene of the worship of the golden calf.
We began to forget about terrible epidemics largely thanks to vaccination, and as vaccinology developed, vaccinations became increasingly safer. For vaccination, weakened pathogens are used, and in recent decades, killed bacteria and viruses or even their purified antigens, which are not capable of causing even the mildest form of infection in the vaccinated person, are increasingly used. However, today new myths about vaccines are increasingly emerging and “anti-vaccination” theories are gaining popularity.
WHO GENERATES MYTHS ABOUT VACCINATIONS?
First of all, individuals involved in health care itself or in related fields are involved in this process. As in any profession, in the medical environment there are competent and not so competent specialists. At the same time, an illiterate physician can give rise to a very harmful myth. Of course, among the most ardent anti-vaxxers, psychopathic individuals predominate, but they are the ones who prefer to be invited to popular talk shows, and it is their illiterate opuses that are willingly published in the press. In their pseudoscientific reasoning, they are able to outshout any intelligent scientist. The horror stories they come up with find an invariable response in the hearts of parents, whose concern for newborns normally reaches an almost paranoid level.
Oddly enough, many myths are supported by the vaccine manufacturers themselves. Vaccines are a very lucrative business and the competition is aggressive. As soon as another myth appears about the mortal danger of one of the components of the vaccine, for example, a preservative, one of the manufacturers immediately replaces this component with an analogue, or finds a way to produce the vaccine without preservatives at all. Moreover, the absence of this component, which is actually completely safe, is used by the manufacturer as a powerful advertising ploy. The average person, hearing that this vaccine is better than all others because it does not contain such and such a preservative, naturally concludes that this component is dangerous to health. Immediately, retrospective analyzes of the health of those vaccinated with old vaccines with the ill-fated preservative begin, and, of course, there are many “victims”...
After scientists started talking about the neurotoxic effect of aluminum, all utensils made from this metal were removed from public catering. “Anti-vaxxers” immediately jumped on vaccine adjuvants. Such adjuvants are presented in a number of vaccines in tiny and completely safe dosages in the form of aluminum alum, which many drink by the spoonful to combat heartburn. You can still find popular aluminum-containing antacids on the shelves of pharmacies. However, many vaccine manufacturers have tried to avoid using aluminum-containing adjuvants, again following myths.

Anti-Vaccination rally in Santa Monica, July 3, 2015 © Kent Nishimura / Los Angeles Times
Several years ago, I encountered a large-scale anti-vaccine protest in Moscow. Leaflets were posted everywhere, convincing passersby of the dangers of the hepatitis B vaccine. The authors of these opuses presented incoherent horror stories based on the fact that this recombinant vaccine is produced from baker's yeast through genetic engineering. “How can this be!” they were indignant: “Scientists want to change our genes!” Nonsense, of course, but many fellow citizens were very scared and refused vaccinations...
About 6 years ago I had the opportunity to give a lecture on tick-borne encephalitis at one of the large enterprises in Siberia. When the topic of vaccination came up, one of the listeners was indignant and told the audience an amazing story. According to her, one of her closest friends gave birth to a child with severe brain underdevelopment due to the fact that shortly before conception her husband was vaccinated against tick-borne encephalitis. It would seem that the whole story is nonsense. But the audience reacted sympathetically to the story. As a result, almost everyone in this group refused vaccination. The more fanciful and categorical a medical horror story, the more followers it has. However, real facts indicate that the vaccines used in medicine today are among the safest drugs, and serious complications after vaccinations are so rare that in most cases it is not possible to prove a cause-and-effect relationship between the vaccine and the disease that occurred at the same time.
Let me give you some numbers:
The childhood measles, rubella, and mumps combination vaccine causes serious complications in 1 in 1,000,000 frail children. At the same time, the measles disease itself can cause the most serious consequences: pneumonia in 6 out of 100 patients, encephalitis in 1 out of 1000, death in 2 out of 1000 children. Rubella causes severe malformations in newborns in every fourth pregnancy complicated by this infection in the first trimester. Mumps (mumps) causes up to 1/4 of all cases of male infertility.
Diphtheria causes death in 1 in 20 cases, tetanus in 2 in 10. Whooping cough kills one in 1,500 children and causes pneumonia in 1 in 8, and encephalitis in 1 in 20. What about the combined vaccine against diphtheria, tetanus and whooping cough ( DPT), not a single case of a fatal complication has been proven, acute encephalopathy is observed in the USA in 0-10.5 cases out of 1,000,000, convulsive and anaphylactic reactions followed by complete recovery are recorded in 1 out of 14,000 cases. To keep the number of severe adverse reactions to an absolute minimum, vaccines are now increasingly using an acellular pertussis component.
The live polio vaccine (oral drops) raises many questions. It is indeed capable of causing vaccine-associated polio in immunodeficient and genetically predisposed children. And although the incidence of such complications is very low (in general, 1 case per 2,500,000 vaccinations), in developed countries pediatricians have switched to an inactivated (killed) vaccine in the form of injections, which does not cause such complications.
How does a button heal?
Some parents begin to panic when they see what processes are happening at the injection site. After all, such complications could simply not have occurred at birth.

7 years after vaccination against tuberculosis, the first symptoms begin to appear 30-45 days after vaccination. The papule heals within 4 – 4.5 months. But after administering the drug, the injection site begins to turn red. Sometimes a bruise appears that turns black, blue, or purple.
This is a normal reaction of the body to the drug. An abscess appears at the site of redness. Under no circumstances should it be crushed or smeared with antiseptics. Over time, the liquid hardens and becomes covered with a thick crust. Then the abscess heals and an almost invisible scar remains on the skin.
Sometimes the abscess bursts and the collected fluid flows out. This is also a normal condition. Liquid may recollect. To get rid of pus, you need to take clean gauze and make a bandage.
After the suppuration stops, a small convex pimple will appear on the skin, which will heal over time and turn into an invisible scar.
EPIDEMICS ARE BACK
The history of vaccine prevention inexorably shows that any interruptions in vaccination of the population against epidemic diseases immediately lead to outbreaks and deaths. Therefore, I do not entirely understand the logic of people calling for a complete refusal of vaccinations.
Let us recall, for example, the recent polio epidemic in Tajikistan, which broke out last spring (wrote here). Flaccid paralysis was diagnosed in 430 Tajik children, and panic reached even Russia. Since paralysis occurs in less than 1% of those infected, it is easy to estimate that up to half a million children were infected. In total, 1 million children at a vulnerable age live in Tajikistan. What does all this mean? Just one thing: the supply of vaccinations to the population in the country is suffering. And this is on the border with Afghanistan, which is unaffected by polio!..
REACTIONS AND COMPLICATIONS DURING VACCINATION
In practice, most post-vaccination reactions are individual in nature and cannot be predicted. Most often, quite predictable mild reactions are observed at the injection site, expressed in swelling and redness of the shoulder and an increase in body temperature to subfebrile levels. Many of these reactions are caused by aseptic inflammation, often due to injection of the vaccine into the subcutaneous fat (especially when vaccinating obese individuals with a short needle). Such reactions go away on their own in a couple of days, and if you take paracetamol, then even faster. Sometimes there is an increase in regional lymph nodes - and this is also a normal reaction to the vaccine.

© ROBIN UTRECHT/AFP/Getty Images
The second most common reaction to vaccination is fainting. Often, from the very sight of the syringe or a few minutes after the injection, vaccine recipients lose consciousness, which is often accompanied by convulsions and vomiting. This reaction is of the same nature as fainting at the sight of blood. It is not related to the vaccine as such, but for an outsider, as well as for the person being vaccinated, such a reaction is very unpleasant. True allergic reactions to vaccine components are relatively rare, but after vaccination the patient should be monitored for an hour in order to react in time to possible anaphylaxis. Before receiving the vaccine, the patient must be asked about his allergies to the components of the vaccine (chicken protein in the influenza vaccine, baker's yeast in the hepatitis B vaccine, etc.).
It should be noted that the presence of contraindications does not mean that the vaccine recipient will inevitably experience a complication. However, contraindications protect the medical worker from possible legal consequences... A clever lawyer can prove to a judge, far from practical medicine, the connection between vaccination and a complication of pregnancy or the birth of a defective child. Therefore, pregnant women are not vaccinated against rubella, mumps, measles, chickenpox and BCG. But non-live anti-influenza vaccines began to be strongly recommended for pregnant women after the swine flu pandemic...
How does the revaccination process work?
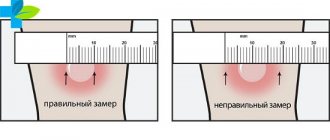
To receive a second vaccination against tuberculosis, the patient must have a negative Mantoux test. Only then can a healthcare worker administer the vaccine.
Vaccination of the population must be done by a medical worker or a doctor with medical education (for example, a nurse or a school doctor).

The vaccination should be done with a new sterile disposable tuberculin syringe and rubber gloves. The needles of such syringes are short and have a thin bevel. But in order to mix the solution, you need to use a long thin needle and another disposable syringe. To do this, the medical worker must unpack the new package, put on gloves, and open the package with the syringe.
The prepared vaccine should be transparent. Before injecting the drug under the skin, you need to make sure that the liquid has not changed color and that no other foreign substances have entered there. If this happens, the drug must be changed. You cannot vaccinate with a drug that has expired. Expired syringes, insulin analogues and needleless injectors are not acceptable.
Before breaking the seal of the package, the medical professional must make sure that the ampoule is not damaged and has a natural color. If the vaccine is sealed under vacuum, the upper part of the ampoule is wiped with alcohol, then the neck is sawed off and broken off.
The sawed part is wrapped in gauze. If there is a ring or a break point on the neck, do not file the ampoule, but press it with your thumb and simply break off the top. All other actions are similar.
To obtain a dose of BCG vaccine ((0.005 ml. in 0.1 ml.), for this, 2 ml of 0.9% sodium chloride solution are injected into one ampoule, which is designed for 20 doses. If the ampoule contains 10 ml., then the amount sodium chloride is reduced by half.
Do not expose the drug to direct sunlight. It is usually covered with a paper cylinder. Once it is dissolved in sodium chloride, its shelf life is no more than an hour.
Before the procedure, the skin is stretched a little, then the drug is partially injected to check whether the needle is positioned correctly. If everything goes well, the procedure is completed.
Popular How to prepare a child for DTP vaccination
A button appears at the injection site (size from 5 to 10 mm). At the very top of the seal it should be white. This is a normal reaction and after 15 - 20 minutes. she disappears.
The injection is administered by a medical professional to the outer part of the left shoulder. It is administered intradermally between the second and third parts of the limb. The drug can be administered subcutaneously or intramuscularly (although there is a risk of a cold abscess). In very rare cases, if the child cannot be injected in the shoulder, it is done in the thigh.

Ability to mix vaccines
It is unacceptable to mix one type of vaccine with other drugs in the same syringe. Moreover, two vaccinations cannot be given at the same time on the same day.
After each injection, the used materials (syringes, gloves, cotton swabs, etc.) are soaked in a special solution (5% chloramine or 3% hydrogen peroxide). Then all this is disposed of.
Revaccinated patients are recorded in a special register. The patient's name, date of the procedure, type of vaccine and manufacturer are entered there. They also add the batch number and expiration date of the solution.
Instruments used for BCG vaccinations are prohibited from being used for other purposes. The drug is stored securely in the refrigerator under a sealed lock.