Measles, clinical picture and course of the disease
The disease begins with an incubation period, which on average in children ranges from 10 to 14 days. During this period, the virus develops latently in the body, so the only criterion by which one can suspect that a child could have become infected is if a measles quarantine was declared at school or kindergarten. In this case, you can protect other children and members of your family who have not been vaccinated against measles by separating them from the child after the 8-9th day of the incubation period for a week (or more if the child is sick).
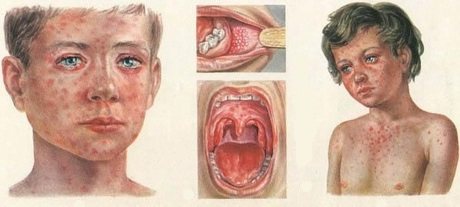
The initial period of measles disease is catarrhal. Since during this period the disease begins acutely with an increase in body temperature to 39 degrees C, a dry, obsessive cough appears in combination with severe conjunctivitis - redness of the mucous membranes of the eyes and “photophobia”. Bright light greatly irritates a person with measles. Cough in the initial period of measles tends to intensify within 3-4 days; in children under 5 years of age there is a high probability of hoarseness, which is the first sign of obstructive laryngitis (in the old terminology - false croup). A cough in a patient with measles is accompanied by a runny nose with copious mucous, and then mucopurulent discharge from the nose, severe general intoxication: weakness, disturbed sleep and decreased appetite.
By the 3rd – 4th day of the disease, the face of a patient with measles takes on a swollen appearance with “swollen” eyelids, red conjunctivae, lacrimation and possible purulent discharge from the eyes.
A typical symptom of measles is described, the so-called Filatov-Koplik spots, which appear at the end of the catarrhal period and 1-2 days before the first skin rash. Filatov-Koplik spots are small whitish-gray dots surrounded by a halo of hyperemia. They are located in the mouth, on the mucous membrane of the cheeks, opposite the molars. In addition to Filatov-Koplik spots in the mouth, red spots may appear on the soft palate, which are called measles enanthema.
The period of rash begins on the 4th – 5th day of the disease with the appearance of maculopapular rash elements on the skin. During this period, intoxication, as a rule, intensifies; the temperature, after some decrease at the end of the catarrhal period, rises again to high numbers. Measles is characterized by a “staged rash.” The first elements of the rash appear behind the ears, on the scalp, as well as on the face and neck. On the 2nd day, the rash covers the torso and arms; on the third day from the onset of the first rash, measles exanthema spreads to the lower part of the torso and legs. The measles rash can be described as bright pink and tends to coalesce into large lesions. The extinction of the elements of the rash also occurs gradually in the same order in which they appeared. In case of late diagnosis, it must be borne in mind that old elements of measles exanthema first turn pale, then acquire a brown color, and remain in this form for quite a long time, up to 10 days. During this final period of measles, the period of pigmentation, fine peeling is also observed on the skin.
In the final period of measles, the symptoms of intoxication and fever subside, and recovery occurs.
How does the disease progress in vaccinated children and adults?
In vaccinated children and adults, measles progresses differently, but in any case does not cause complications.
Much depends on the concentration of antibodies to the virus in the body and general health. As a rule, in vaccinated people, signs of measles pathology appear on the tenth day after infection.
In most vaccinated children and adults, measles occurs in an atypical form. Catarrhal and intoxication symptoms are mild.
The temperature throughout the illness sometimes remains at 36.6-37 degrees. The rash often appears immediately in spots of light pink color. Rashes on the body are sporadic, quickly fade and disappear.
Post-measles pigmentation is noticeable for no longer than a week. In weakened vaccinated individuals with low concentrations of antibodies in the blood, measles may be more severe.
Preventing measles
The main method of preventing measles is active immunization, that is, measles vaccination, which, according to the mandatory vaccination calendar approved in the Russian Federation, is carried out in children aged 12 months and 6 years, as well as adults under 35 years of age who have not had measles.
Unfortunately, the practice of “unreasonable medical withdrawals”, and frankly speaking, the unwillingness of some parents to get vaccinated in the case of measles, is already leading to very negative consequences. In 2011, an outbreak of measles was recorded in Moscow, the source of which was an adult who worked in a children's team (not a health worker), and as a result, children with young mothers were infected in several children's hospitals, where infants were taken from a children's institution in the catarrhal period of measles infections with a diagnosis of ARVI, when measles-specific rashes on the skin and mucous membranes, as you and I now know, do not yet exist. Every year, cases of epidemic outbreaks of measles are recorded in cities of the Russian Federation. Given the high mobility of the population, including children in large cities, unfortunately, no one is immune from contact with a person with measles. A timely measles vaccination significantly reduces the risk of getting sick from accidental contact in public places, but if, by an unfortunate coincidence, there is close contact with a relative or friend who is at an early stage of measles infection, then the presence of post-vaccination immunity reduces the likelihood of a moderate or severe course measles in a vaccinated person is approximately 80%, and in a child with good immunity it is almost 100%. In other words, vaccinated children usually suffer from measles in a mild form, unlike unvaccinated children, who always get seriously ill, and some also suffer the serious complications mentioned above.
Is a vaccinated person contagious to others?
To protect against measles, children and adults are given vaccines containing live inactivated viruses. People for whom vaccination is strictly contraindicated for health reasons are interested in whether a vaccinated person is capable of infecting others.
Theoretically, this is possible, since the drug contains a live pathogen. But in practice, no cases of infection from a recently vaccinated patient have been recorded.

A vaccinated person can be infectious to others in the following cases:
- his body is weakened and cannot cope with the inactivated measles pathogen introduced. As a result, a real viral pathology began to develop;
- for some reason, specific immunity was not formed. The person came into contact with a person with measles, became infected and became a carrier of the virus.
After vaccination, some patients do not have sufficient antibodies in their blood. There are a number of reasons for this:
- a spoiled vaccine was used;
- the body did not respond to the vaccine due to individual characteristics;
- Doctors administered the drug incorrectly.
When asked whether there is a chance of contracting measles from a vaccinated person, doctors answer differently. Some argue that this is impossible because the virus is weakened in the vaccine.

For example, pediatrician Komarovsky believes that there is no need to be afraid of immunized children, because they have been injected with a neutralized measles pathogen, which cannot be transmitted by airborne droplets.
Other doctors say there is a risk of infection, especially in weakened people.
Therefore, it is better not to put yourself in danger and not communicate for some time with a person who has recently been vaccinated.
It is especially recommended to avoid contact with the vaccinated person for young children, pregnant women, and people with immunodeficiency.
Features of the course of measles in adults
WHO experts believe that the incidence of measles in Europe has reached a historic high over the past ten years. The measles situation in the world, including in European countries, has remained unfavorable for three years now. In the first six months of 2021, more than 41 thousand cases of measles in children and adults were reported in the region, of which 37 episodes were fatal. The European Center for Disease Prevention and Control associates this frightening trend with a decrease in the global vaccination rate to 78% instead of the required 90–95% [1]. Today, measles continues to spread throughout Russia. According to Rospotrebnadzor of the Russian Federation, for the first half of 2021, the incidence of measles increased 13.5 times compared to the same period in 2021 and amounted to 1.17 per 100 thousand people, the number of cases was 1,717 [2]. WHO calls on all countries to take decisive action to stop the epidemic, mainly through control of population vaccination, and all regions have once again set the goal of eliminating measles by 2021 [1, 2].
Measles is a highly contagious anthroponotic viral infection with an aspiration mechanism of pathogen transmission. It is characterized by febrile, intoxication and exanthema syndromes, the presence of catarrhal phenomena, enanthema and often occurs with primary and/or secondary complications. The causative agent of measles is an RNA genomic virus belonging to the paramyxovirus family. The pathogen is unstable in the environment, but it can remain alive for several hours in aerosols. In terms of its epidemiology, measles is a typical droplet infection. The source of infection is sick people. The greatest danger in terms of transmission of infection is posed by patients in the catarrhal period (on average 4 days before the appearance of the rash and up to the 5th day from the appearance of the rash). The incubation period for measles is most often 10–14 days.
One of the most dangerous viral infections for adults is measles, the contagiousness index (morbidity after contact with the pathogen) is 90–95%, and the disease is much more severely tolerated by adults than by children. At the onset of measles, damage to the epithelial cells of the respiratory tract dominates with the development of corresponding clinical manifestations. The measles virus, located in the mucous membrane of the upper respiratory tract and in the nasopharyngeal mucus, is released from the body when coughing, sneezing, talking and even breathing in the form of tiny aerosol droplets. Measles symptoms do not appear immediately after infection. The classic clinical course of measles is divided into periods: incubation (from 7 to 21 days), catarrhal (the first symptoms of measles appear: increased body temperature, cough, runny nose) and periods of rash, pigmentation and recovery (convalescence) [3].
The first manifestations of measles (prodromal stage) are nonspecific symptoms: fever, cough, runny nose, conjunctivitis. At the end of the prodromal period, Belsky-Filatov-Koplik spots appear on the buccal mucosa, which are specific for measles. They look like gray-white grains surrounded by hyperemia, located at the level of the second molars. These rash elements persist for several days and begin to disappear when rashes appear on the skin. Measles rashes are characterized by stages: first, the rash appears on the face, behind the ears, on the scalp, then moves to the torso and arms, and then spreads to the legs. Morphologically, the rashes have an erythematous, maculopapular appearance. The rash lasts up to 5 days, then it fades away, leaving behind pigmentation that disappears within 2-3 weeks. Simultaneously with pigmentation, pityriasis-like peeling appears, most pronounced on the face and torso.
Measles can have typical or atypical presentations. Atypical include:
- Erased form. In this case, the disease occurs in a very mild form, without pronounced specific clinical manifestations. Patients note a slight increase in body temperature and cold symptoms (sore throat, cough, weakness). Sometimes an erased form of the disease occurs after measles vaccination or administration of gamma globulin.
- Hemorrhagic form, when the disease is accompanied by multiple hemorrhages on the skin, an admixture of blood in the urine and stool. Due to the hemorrhagic form, death often occurs due to large blood loss. With timely hospitalization and proper treatment, the prognosis of the disease is favorable.
- Hypertoxic form , which occurs against the background of severe intoxication of the body and is manifested by temperatures up to 40 ° C and above, symptoms of meningoencephalitis, cardiac and respiratory failure [3].
Atypical manifestations are more common in adults. The course of measles in adults has its own characteristics: intoxication syndrome is more pronounced (weakness, sweating, drowsiness, lethargy); Of the catarrhal phenomena (nasal congestion, conjunctivitis, cough, sore throat and discomfort in the throat), a dry cough often predominates and there is a violation of the phasing of rashes.
Measles in adults is diagnosed based on characteristic symptoms and laboratory results. According to clinical recommendations, serological and molecular biological methods are used for laboratory diagnosis of infection. A blood test is carried out using an enzyme-linked immunosorbent assay (ELISA), and to determine antibodies (IgM, IgG) to the measles virus, blood is taken on the 5th day from the onset of the rash [4]. To identify and determine the type of virus, the polymerase chain reaction (PCR) method is used. To conduct the study, material is collected (nasopharyngeal swabs, urine, cerebrospinal fluid) 1–3 days after the rash. In some cases, special virological diagnostic methods are used (virus microscopy, immunofluorescence reaction).
A general blood test for measles is characterized by a decrease in the number of leukocytes and an increase in the erythrocyte sedimentation rate. If a secondary bacterial infection occurs, neutrophilic leukocytosis is noted in the study results. It is also recommended to perform a biochemical blood test and a general urine test: they will help determine the presence and severity of damage to the liver and urinary system. When managing a patient with measles, monitoring clinical and biochemical blood tests over time is mandatory. If necessary, additional diagnostics are carried out - analysis of cerebrospinal fluid, radiography and computed tomography of the chest organs, electrocardiography (ECG), consultations with an ENT doctor, neurologist and other specialists as indicated.
A feature of the interaction between the measles virus and the human immune system is the development of transient secondary immunodeficiency [5], which implies a high risk of severe complications (bacterial and/or viral etiology), which can be destructive. Acute and chronic diseases of the ENT organs occur more often, the most common of which is otitis media, occurring in 7–9% of patients; lesions of the digestive system (enterocolitis, diarrhea, hepatitis, pancreatitis) and the urinary system (pyelonephritis, cystitis, glomerulonephritis), as well as diseases of the central nervous system, most often occurring in the form of acute infectious and post-infectious encephalitis with a frequency of 0.01–0.02%. Complications are observed in the form of infectious pathology of the lower respiratory tract, where pneumonia occurs in 1–6% of patients and can be of either viral or bacterial etiology. Symptoms such as constant unmotivated weakness, headaches, the presence of a dry cough, changes in the auscultation pattern, prolonged fever and a repeated increase in temperature make it possible to be wary of the presence of pneumonia. An objective picture is provided by computed tomography of the chest organs; a bacteriological examination of sputum should also be carried out (in the presence of a wet cough, with the correct and correct collection of biomaterial), PCR testing for respiratory viruses and bacteria to clarify the etiology.
There is no specific treatment for measles, so therapy for this infectious disease is aimed at alleviating the patient’s condition and combating secondary infections and complications. The patient is prescribed antipyretic drugs to reduce the temperature and eliminate the symptoms of intoxication and inflammation. For etiotropic therapy, it is recommended to use interferons (interferon-alpha) and normal human immunoglobulin in severe forms of infection. For detoxification therapy for moderate and severe forms, electrolyte solutions are indicated; for mild cases, oral rehydration is used. Symptomatic therapy is aimed at relieving symptoms (decongestants, antitussives and expectorants, antipyretics, antihistamines). If complications develop, therapy is carried out aimed at preventing them, including antibacterial therapy [6]. Such groups of antimicrobial drugs as macrolides and fluoroquinolones of the III and IV generations are preferable for pneumonia caused by mycoplasma and chlamydial infections, while bacterial pneumonia (streptococcal, staphylococcal, etc.) with measles can be successfully treated with beta-lactam antibiotics [ 6, 7].
In January 2021, patients from a family outbreak of measles were admitted to the State Budgetary Healthcare Institution No. 2. Patients from the Roma community were hospitalized. After the first sick patient from a family unit was hospitalized with a confirmed diagnosis of measles, contact persons refused specific prophylaxis, which contributed to a measles outbreak in the community. Several sick people refused hospitalization. A typical course was observed in only one patient of the cases. Three patients out of 4 hospitalized patients had no rash, fever syndrome predominated, and the fourth patient had a complicated course of measles, a clinical example of which is given below.
Patient X., 20 years old, was hospitalized from 01/18/18 to 01/26/18 with a diagnosis of “Measles, moderate severity. Complication: community-acquired left-sided upper lobe pneumonia. DN 0".
The patient fell ill on January 16, 2018, when his body temperature began to rise to 40 °C. The patient denied catarrhal symptoms. He took antipyretic drugs and carried out symptomatic therapy, but did not remember the names of the drugs. The fever persisted for two days, and there was no effect from taking the medications. On 10/18/18 he called an ambulance team and was hospitalized at the IKB No. 2.
From the epidemiological history it was found that the patient had contact with relatives at the outbreak, some of whom were hospitalized with a diagnosis of measles. The patient had no information about vaccinations and refused vaccination before becoming ill.
Upon admission, the patient was in a state of moderate severity, with a fever of up to 40 °C; according to an objective examination, the skin was physiologically colored, moist, hot to the touch, clean, and there was no rash. The sclera is not injected. The mucous membrane of the oral cavity is not hyperemic. The tonsils are not hyperemic, not enlarged, without overlap. The tongue is clean and moist. Small cervical lymph nodes were palpated, up to 1 cm, elastic, painless on palpation. Nasal breathing is free. In the lungs, breathing is harsh, carried out in all departments, wheezing was not heard. Heart sounds were clear, rhythmic, heart rate and pulse were 78 beats per minute. Blood pressure 100/60 mm Hg. Art. The abdomen on palpation is soft, painless in all parts, the liver and spleen are not enlarged. The Shchetkin–Blumberg symptom is negative. Urination is free, painless, urine color is yellow, diuresis is sufficient. The stool is regular, formed, without pathological impurities. Severe meningeal and focal symptoms were not identified.
A laboratory and instrumental examination was carried out in the form of a general blood test - leukocytes 5.7, neutrophils 68 (band - 1, segmented - 67), lymphocytes 19, monocytes 13, erythrocytes - 5.25, hemoglobin 157; ESR - 5 mm/h; biochemical blood test - total protein 69.1 g/l, ALT 31 U/l, AST 49 U/l, urea 3 mmol/l, creatinine 107 µmol/l, glucose 5.9 mmol/l; HIV test and markers of viral hepatitis B and C are negative; ELISA with measles antigens in GORSES - positive, chest x-ray - the pulmonary pattern is enhanced, in the projection of the upper parts of the left lung a small zone of peribronchovascular infiltration of lung tissue is visualized without clear contours, low intensity. Treatment was carried out: intravenous detoxification therapy with crystalloid solutions, desensitizing therapy, vitamin therapy, antitussive therapy, antibiotic therapy with cefotaxime and azithromycin. During the treatment, on the 3rd day of hospitalization, the body temperature returned to normal, and the patient noted an improvement in health. On the 8th day of hospitalization, the patient underwent repeated radiographic monitoring of the chest organs, and positive dynamics were observed. The patient was discharged with improvement under outpatient supervision.
The given clinical example confirms that measles can often be more severe and with complications in unvaccinated individuals.
According to O. V. Tsvirkun [8], measles outbreaks predominantly formed in hospitals (59%), in families (40%), less often (1%) at the place of residence or in orphanages, which indicates the need for more careful compliance with the rules epidemic surveillance, timely identification and isolation of the patient, as well as careful monitoring of contacts, timely immunoprophylaxis [9].
When isolating a patient at home, daily wet cleaning is required, if possible, limiting the patient’s contact with family members as much as possible, and prohibiting the patient from visiting relatives or friends. All contacts are subject to medical observation until 21 days from the moment the patient is identified [10].
Hospitalization of patients is carried out in case of severe disease and for epidemic indications (persons living in dormitories, hotels, hostels, etc., decreed groups of people). Patients are hospitalized in a separate room and subject to strict bed rest. Persons hospitalized in a hospital must be discharged no earlier than 5 days from the moment the rash appears. Medical personnel who come into contact with a patient with measles are required to observe all safety measures before visiting the box: be vaccinated or have a high protective titer of antibodies, be sure to wear a cap, gloves, masks and special medical clothing.
After discharge from the hospital or treatment in isolation at home, patients are subject to mandatory dispensary registration at the place of attachment to the clinic for a period of 1 month. The frequency of mandatory control examinations by a doctor is once every two weeks. Blood and urine tests are carried out after 2 and 4 weeks, respectively, ECG and other laboratory and instrumental research methods are carried out as indicated, as well as consultations with specialists [10]. After 1 month of medical supervision, if there are good laboratory parameters and no complications, the patient must be removed from the dispensary register.
It is well known that the most important and effective way to prevent measles is vaccination. The main and only correct method of preventing the disease is active immunization. High-quality vaccination carried out according to the terms of the National Vaccination Calendar in compliance with all standards, and regular revaccination, an increase in protective antibody titers lead to the impossibility of contracting the infection, and persons vaccinated once, as a rule, suffer a mild or atypical form of the disease [11, 12].
The vaccine is given to children who have not had measles from the age of 12 months. Revaccination is carried out once at 6 years of age, before entering school. Adolescents and adults under 35 years of age who have not been sick, have not been vaccinated, and have been vaccinated once and do not have information about preventive vaccinations against measles are also subject to immunization against measles. The duration of post-vaccination immunity is up to 8–10 years [13]. It is recommended to revaccinate every 10 years in patients with a low titer of protective antibodies.
In the Russian Federation, the use of the LIV Ruvax (Aventis-Pasteur, France), the complex vaccine against measles, rubella and mumps M-M-R II (Merck Sharp Dome, USA), Priorix (GlaxoSmithKline, England) and etc. Children who have not been vaccinated against measles or mumps (have not reached vaccination age or have not received vaccination due to medical contraindications or refusal to vaccinate) no later than the 5th day from the date of contact with a measles patient, as well as persons vaccinated against measles once - without age restrictions, normal human immunoglobulin is administered in accordance with the instructions for its use [10]. Passive prevention of measles in adults is carried out by administering immunoglobulin, which is obtained from donor plasma. For greatest effectiveness, the drug is administered no later than 72 hours after contact with the patient. According to epidemic indications, immunization against measles is required for persons who had contact with the patient during the first 72 hours from the moment the patient was identified (if the disease is suspected), who have not had measles before, who have not been vaccinated, and who do not have information about vaccinations. If the boundaries of a measles outbreak expand (at a place of work, school, within a district, a settlement), the immunization period can be extended to 7 days from the moment the first patient in the outbreak is identified. In a timely manner, it is imperative to isolate the sick family member in a separate room, provide him with an individual set of dishes, bed linen and care.
As non-specific preventive measures, it is recommended to wear a medical mask in public places (metro, shops and shopping centers, prefectures, clinics), especially during the epidemic season, maintaining a healthy lifestyle, a balanced diet high in proteins and vitamins, observing a work and rest schedule, hardening, avoiding hypothermia and drafts. Timely treatment of chronic diseases is necessary, which contribute to the deterioration of the immune system and increased susceptibility to pathogenic bacteria and viruses.
Conclusion
Timely identification and isolation of patients, correct hospitalization according to clinical and epidemiological indications, competent tactics for managing the patient and contact persons will help stop the growth of morbidity and transmission of infection, prevent the risk of complications and deaths, and active vaccine prevention of the population with wide immunization coverage will lead to complete elimination and elimination measles
Literature
- Measles. World Health Organization. https://www.who.int/ru/news-room/fact-sheets/detail/measles.
- Information on infectious and parasitic diseases for January-June 2021. Infectious morbidity in the Russian Federation for January-June 2021. Federal Service for Surveillance on Consumer Rights Protection and Human Welfare. https://rospotrebnadzor.ru/activities/statistical-materials/statictic_details.php? ELEMENT_ID=10419.
- Ponezheva Zh. B., Arakelyan A. K., Kozlova M. S., Vdovina E. T. Measles in adults // Epidemiology and infectious diseases: current issues. 2021. pp. 50–55.
- Lobzin Yu. V. Clinical recommendations (treatment protocol) for providing medical care to children with measles. St. Petersburg, 2015. Paragraphs 4.7, 4.11.
- Yushchuk N. D. Viral diseases. Tutorial. M.: GEOTAR-Media, 2016. 640 p.
- Dementiev A. S. (compiled). Airborne infections. Standards of medical care. M.: GEOTAR-Media, 2021. 448 p.
- Stetsyuk O. U., Andreeva I. V. Popular myths and misconceptions regarding antibiotics among practicing doctors // Russian Medical Journal. 2014. No. 9. pp. 684–692.
- Tsvirkun O. V., Gerasimova A. G., Tikhonova N. T., Ezhlova E. B., Melnikova A. A., Dubovitskaya E. L., Orlova O. S., Basov A. A., Frolov R. A. The incidence of measles in different age groups during the period of elimination of infection // Epidemiology and vaccine prevention. 2017. pp. 18–25.
- Prevention of measles, rubella, mumps. Sanitary and epidemiological rules SP 3.1.2952–11, 2012
- Golovko M. G., Poryadina G. I., Larina V. N. Measles in the practice of a clinic therapist // General Medicine. 2014. No. 4. pp. 10–16.
- Lobzin Yu. V. Guide to infectious diseases. St. Petersburg, 2000. P. 93.
- Karen Gill. Understanding the causes of meats. MD - Medical News Today, 05/15/2017. https://www.medicalnewstoday.com/articles/37135.php.
- Warning about the dangers of meats may sway vaccine skeptics - Published By Honor Whiteman - Medical News Today, 4 August 2015. https://www.medicalnewstoday.com/articles/37135.php.
I. A. Ivanova*, 1 Zh. B. Ponezheva*, Doctor of Medical Sciences M. S. Kozlova** E. T. Vdovina**, Candidate of Medical Sciences N. A. Tsvetkova**, Doctor of Medical Sciences, Professor
* Federal Budgetary Institution Central Research Institute of Energy of Rospotrebnadzor, Moscow ** GBUZ IKB No. 2 DZM, Moscow
1 Contact information
Features of the course of measles in adults / I. A. Ivanova, Zh. B. Ponezheva, M. S. Kozlova, E. T. Vdovina, N. A. Tsvetkova For citation: Attending physician No. 11/2018; Page numbers in the issue: 36-39 Tags: viral infection, infection, adults, clinical example
What complications does measles cause?
A third of patients develop an upset stomach, conjunctivitis, and may develop inflammation of the middle ear. Pneumonia and meningitis occur less frequently.
It is extremely rare (up to 4 cases per million cases) that within several years after measles, a person may develop a brain disease that leads to irreversible changes in the central nervous system, including seizures and mental impairment.
In children under 5 years of age, complications occur less frequently than in patients over 20 years of age and in people with weakened immune systems. The mortality rate from measles among children is low: 1 case in 1000 is fatal.
How does measles spread?
The virus spreads through the air, the current from which can even reach another floor through ventilation pipes. In a closed, cramped room, it easily affects the respiratory tract, mucous membrane of the throat and eyes. It also enters the body with droplets of saliva from a sick person when he sneezes or coughs. Sunlight quickly kills the measles virus. Disinfection of the room in which sick children were located is not required; good ventilation is sufficient, since the lifespan of the virus is only 2-3 hours at normal temperature.
If a child is not vaccinated on time, then in close contact with a sick person he will definitely get sick. The virus reaches its peak development towards the end of the incubation period and over the next few days. It is at this time that the patient is contagious to others and should not have contact with other children or attend kindergarten or school.
The measles virus, during its life processes, produces toxic substances that poison the body of children. A symptom of measles is a characteristic red rash on the face and body.
Danger of disease
Previously, it was believed that only children were susceptible to the measles virus. Due to the high mortality rate (every 4th child who fell ill in Russia died!), the disease was popularly called the “children's plague.” In the 21st century, the situation has changed, and now adults are more likely to suffer from measles. Among the sick are people who have not been vaccinated and who did not have measles in childhood.
In the modern world, the number of cases of measles has decreased hundreds of times, which became possible thanks to immunization. However, the disease has not disappeared completely, and cases of infection are still being reported in different countries. The virus easily travels long distances, so it is not necessary to be in close contact with an affiliated person: you can get sick even if you are several tens of meters from the patient. Adults get measles more severely than children and are more likely to experience complications. The virus enters the body through the respiratory system and mucous membranes. It affects the respiratory, nervous and gastrointestinal systems. A vaccinated person can also get measles, but in this case the disease will be relatively mild.
Preventive measures
Prevention of measles in children includes several important points.
- Vaccination. The most effective protection is a vaccine. It can be single-component or multi-component (MMR, or measles, mumps, rubella). The vaccination is carried out at 1 year, then again at 6 years. Up to 10% of vaccinated children may develop a mild form of infection with a minor rash and fever. At this point, children are considered not contagious. Due to the massive refusal of vaccinations in Russia, cases of measles have become more frequent. According to statistics, 80% of children who suffered from this disease were not vaccinated.
- Taking immunoglobulin, or passive immunization. If it is known that the child had contact with a carrier of measles or was in an outbreak of the disease, immunoglobulin can be used, which provides immunity from infection for one month.
- Quarantine. In the children's group where a case of measles was recorded, anti-epidemic measures and daily preventive examination of children are carried out. A child is considered contagious several days before the first symptoms appear, as well as for 5 days after the first skin rash appears. Staying in a children's group is prohibited. Quarantine is carried out only for unvaccinated children under 17 years of age.
Recurrence of measles occurs in extremely rare cases. After an illness, immunity is lifelong. After vaccination, stable immunity remains for 15 years.
Illness in early childhood
Features of the course of measles in young children:
- Children under three months of age cannot become infected with measles - this is due to the fact that their mother passed on her immunity to them at birth. The woman herself was either vaccinated against measles or had it.
- Passive immunity, which lasts up to 6 months, protects infants at this age and they become infected extremely rarely.
- For early childhood, the atypical form of measles is more typical. There is a shortened catarrhal period, mild symptoms, the absence of Filatov-Koplik spots and enanthems on the oral mucosa. Sometimes the incubation period is replaced by a rash, and the catarrhal period is completely skipped.
- Although the symptoms in early childhood are not as severe, measles often causes complications. This is due to the fact that a weak immune system does not always know how to fight back a powerful virus that suppresses all the body’s defenses.

How to treat measles?
There are no special treatments for measles; the body will cope with the infection on its own. Treatment of the child here is symptomatic, which will alleviate the general condition of the patient:
- Antihistamines. Prescribed to relieve swelling of the nasopharyngeal mucosa.
- Antipyretic. It is recommended to use drugs based on paracetamol and ibuprofen.
- Vitamin therapy. With measles, vitamin metabolism is disrupted and the body's protective properties are significantly reduced. Your doctor may prescribe vitamin C and a vitamin complex.
- Cool damp air in the room. Helps moisturize mucous membranes, cough becomes less dry.
- Hygiene procedures. During the recovery period, you can take baths. It is also necessary to carry out thorough oral hygiene and wash the eyes if there is an inflammatory process.
- Diet. After the acute period, when the temperature subsides, the child develops an appetite. Light, pureed, warm food should be offered.
During illness, it is also important to provide the child with the necessary vitamin complexes to maintain immunity, and to lubricate chapped lips with Vaseline.
A patient with measles needs bed rest while the temperature persists. If possible, give him a separate room. Wet cleaning should be carried out at least 2 times a day. It is very important that the air remains fresh at all times, so ventilate the room more often. If bright light causes discomfort, then close the curtains and in the evening turn on a table lamp instead of a chandelier. Follow a daily routine. Although sleep is disturbed and insomnia has appeared, try to go to bed on time. This is especially true for children. If it is difficult to keep your child in bed, then allow him to play quiet games, watch a little TV, or read together. But it is advisable that he sleep after lunch.
Symptomatic treatment is carried out at home under the supervision of a pediatrician. The child is admitted to the hospital department if complications begin to develop. If there are complications, therapy is supplemented with antibacterial drugs.