Injections into the subcutaneous fat layer are recommended when rapid action of the active substance is required. Due to the good supply of blood vessels to the area, such injections ensure rapid absorption of the drug, regardless of the injection site. This technique is used for courses of hormonal drugs, oil solutions, fat-soluble vitamins, insulin, heparin, and other drugs.
Rules for administering subcutaneous injections
Subcutaneous injections are given for therapeutic and prophylactic purposes to a depth of 1.5 cm with syringes with a volume of 1-2 ml (the optimal needle length is 2 cm) in the following areas:
- outer surface of the shoulder and thigh;
- anterior abdominal wall;
- under the shoulder blade.
In these areas, the skin is easy to fold, and the likelihood of damage to nerves, blood vessels and periosteum is minimal. Rapid absorption of the drug in loose fiber minimizes the effect of the drug on the entire body.
Oil solutions are classified as poorly absorbed drugs, so they are administered after preheating to 38 degrees. Afterwards, you need to apply a heating pad or a warming compress to the injection site. These precautions will prevent the formation of infiltrates.
It is not recommended to administer injections in areas with swollen subcutaneous tissue, as well as in areas of compaction after previous injections. Following the correct technique ensures the safety and effectiveness of therapy.
Injections
Injection is the introduction of medicinal substances using special injection under pressure into various environments of the body. There are intradermal, subcutaneous, intramuscular and intravenous injections. For special indications, intraarterial, intrapleural, intracardiac, intraosseous, and intraarticular administration of drugs is also used. If it is necessary to achieve a high concentration of the drug in the central nervous system, spinal (subdural and subarachnoid) administration is also used.
Injection methods of administering drugs are used in situations where a quick effect is needed, for example, in the treatment of emergency conditions. This ensures a high rate of entry of medicinal substances into the blood and the accuracy of their dosage, and the required concentration of the drug in the blood is maintained for quite a long time thanks to repeated injections. The injection method is also used in cases where it is impossible or impractical to administer the medicine orally or there are no appropriate dosage forms for oral administration.
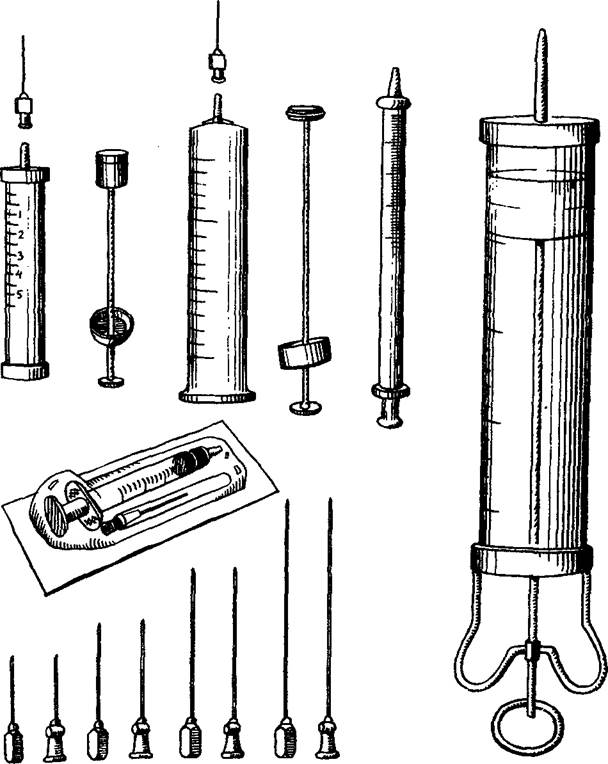
Rice. II. Types of syringes and needles.
Injections are usually given using syringes and needles. Syringes of various types (Record, Luera, Janet, shown in Fig. 11) consist of a cylinder and a piston and have different volumes (from 1 to 20 cm3 or more). The thinnest are syringes for administering tuberculin; their division price is 0.02 ml. Special syringes also exist for administering insulin; The divisions on the cylinder of such syringes are marked not in fractions of a cubic centimeter, but in units of insulin. Needles used for injections have different lengths (from 1.5 to 10 cm or more) and different lumen diameters (from 0.3 to 2 mm). They must be well sharpened
Currently, so-called needle-free injectors are used, which allow the administration of a medicinal substance intradermally, subcutaneously and intramuscularly without the use of needles. The action of a needleless injector is based on the ability of a jet of liquid supplied under a certain pressure to penetrate the skin. This method is used, for example, for pain relief in dental practice, as well as for mass vaccinations. The needle-free injector eliminates the risk of transmitting serum hepatitis and is also characterized by high productivity (up to 1600 injections per hour).
Syringes and needles used for injections must be sterile. To destroy microbial flora, various sterilization methods are used, most often based on the action of certain physical factors.
The most optimal and reliable methods are sterilization of syringes and needles in an autoclave using saturated water steam under a pressure of 2.5 kg/cm2 and a temperature of 138 °C, as well as sterilization in a drying-sterilization cabinet with dry hot air. In everyday medical practice, boiling syringes and needles is still sometimes used, which, however, does not ensure complete sterilization, since some viruses and bacteria are not killed. In this regard, disposable syringes and needles seem ideal, providing reliable protection against HIV infection, hepatitis B and C.
Sterilization by boiling requires compliance with a number of rules and a certain sequence in the processing of syringes and needles. After performing the injection, the syringe and needle are immediately washed with cold running water to remove any remaining blood and medication (after they dry, this will be much more difficult to do). Disassembled needles and syringes are placed for 15 minutes in a hot (50 ° C) washing solution prepared at the rate of 50 g of washing powder, 200 ml of perhydrol per 9750 ml of water.
After thorough washing in the specified solution using brushes or cotton-gauze swabs, the syringes and needles are rinsed a second time in running water. Then, in order to check the quality of the treatment, samples are taken selectively to detect blood and detergent residues in needles and syringes.

The presence of traces of blood is determined using a benzidine test. To do this, mix several bepzidine crystals with 2 ml of a 50% acetic acid solution and 2 ml of a 3% hydrogen peroxide solution. A few drops of the resulting solution are added to a syringe and passed through a needle. The appearance of a green color indicates the presence of blood residues in the instruments. In such cases, syringes and needles need to be reprocessed to avoid the transmission of various diseases (for example, serum hepatitis, AIDS).
Detergent residues are determined using a sample with
Rice. 12. Placing syringes in the sterilizer.
| Rice. 13. Sequence of syringe assembly. |
phenolphthalein. The main reaction produced by the cleaning solution is responsible for the appearance of a pink color after the addition of a few drops of a 1% phenolphthalein solution. Boiling of syringes and needles is carried out in a sterilizer. Disassembled syringes are wrapped in a gauze cloth, placed together with needles, mandrels, tweezers, hooks on its metal grid (Fig. 12), filled with distilled or boiled water and boiled for 45 minutes. Then remove the sterilizer lid and place it on the table with the outer surface. Use a sterile forceps to remove hooks that lift the sterilizer mesh and place it
across. The syringe is collected with tweezers; They also put on and secure the needle (Fig. 13).
Currently, in accordance with current instructions, boiling as a method of sterilization in medical institutions is no longer used (except in cases where for some reason it is impossible to use other sterilization methods), giving way to sterilization in a drying-sterilization cabinet and an autoclave.
When sterilizing with hot air in a drying-sterilization (dry-heat) cabinet (at a temperature of 180 ° C for 1 hour) and water steam in an autoclave (for 20 minutes), after pre-sterilization treatment, dry syringes (disassembled!) and needles are placed in bags made of special paper (kraft bags). The packages indicate the capacity of the syringe and the date of sterilization. The bags are placed in a dry-heat oven or steam sterilizer. Sterilization control is carried out in the first case with the help of sucrose, which, when the required temperature is reached, turns from a white crystalline powder into a dark brown mass, and in the second case, with the help of benzoic acid, the crystals of which melt at the sterilization temperature.
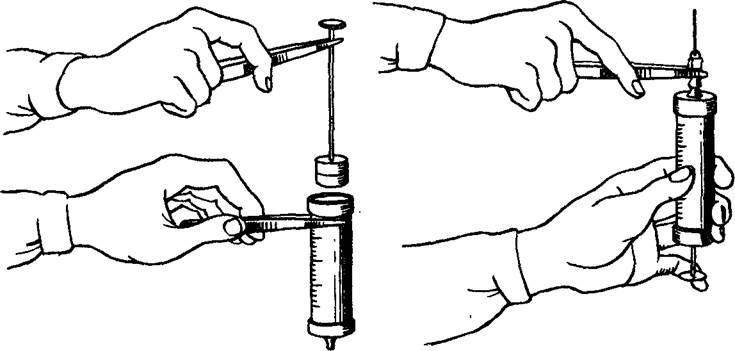
Before you draw medicine from a bottle or ampoule into a syringe, you need to check its name and make sure the drug is ready. The neck of the ampoule or the cap of the bottle is wiped with alcohol, the ampoule is opened, after which its contents are drawn into a syringe with a separate needle. Then this needle is removed and another one is put on, with which the injection is performed. If it is necessary to carry out an injection in the ward, the syringe with the collected medicine is brought there in a sterile tray along with cotton balls moistened with alcohol.
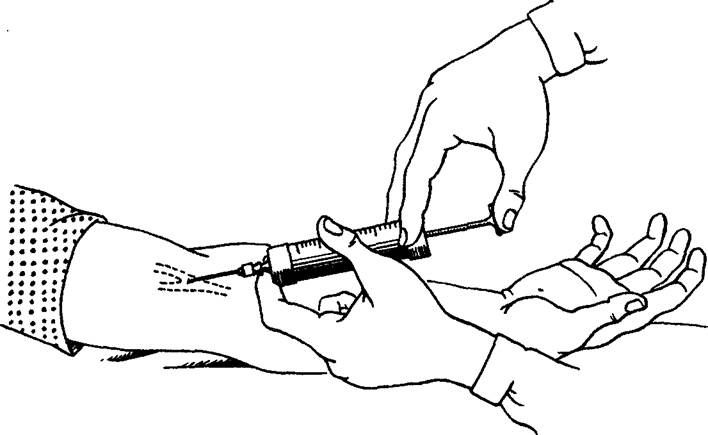
7.2.1.1. Intradermal injections
Intradermal injections are used for diagnostic purposes to perform the tuberculin Mantoux reaction, various allergy tests, as well as in the initial stages during local anesthesia. To perform intradermal injections, the inner surface of the forearm is usually chosen. It is necessary that the needle (preferably short) enters the skin to a shallow depth (until its lumen disappears), after which the contents of the syringe are injected at an acute angle. With the correct technique, a “lemon peel”-shaped bump remains at the site of the intradermal injection.
Rice. 14. Areas of the body for subcutaneous injections.
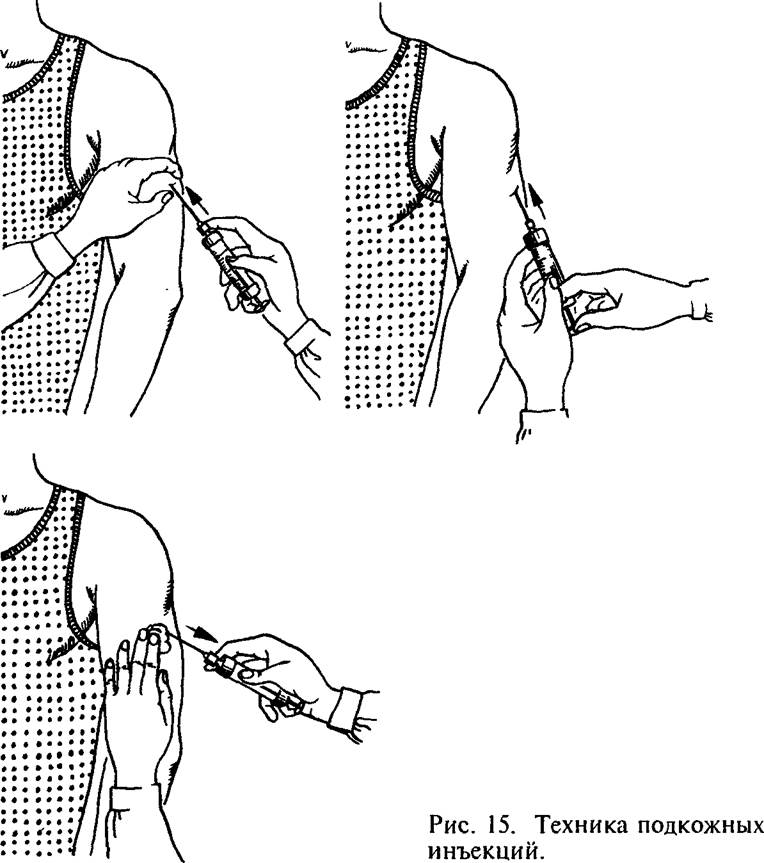
7.2.1.2. Subcutaneous injections
Using subcutaneous injections, medicinal substances are administered that are well absorbed in the loose subcutaneous tissue. The most convenient place for subcutaneous injections is the outer surface of the shoulder and thigh, the subscapular region; for the administration of some drugs (for example, heparin) - the lateral surface of the abdominal wall (Fig. 14). After thoroughly treating the skin with a cotton ball with alcohol, a skin fold is formed with the left hand, and the prepared syringe is taken with the right hand, after which a needle is inserted into the base of the resulting triangle approximately one-third of its length. After puncturing the skin, the syringe is transferred to the left hand and its contents are slowly injected. Then the needle is quickly removed, and the injection site is again wiped with alcohol and pressed with a cotton ball (Fig. 15).
In addition to subcutaneous injections, subcutaneous infusions using systems for drip administration of solutions were used quite widely in the past (see 7.2.1.4 - Intravenous injections and infusions). Currently, this method is used relatively rarely, since with its help it is possible to administer no more than 400-500 ml at a time
liquids. Some solutions (for example, calcium chloride, hypertonic sodium chloride solution) cause necrosis of subcutaneous fat when injected subcutaneously. Finally, compared to intravenous infusions, subcutaneous infusions are less effective in resuscitation.
7.2.1.3. Intramuscular injections
Medicines administered intramuscularly are absorbed faster than with subcutaneous injections. For intramuscular injections, places where the muscle layer is quite well developed are most often chosen: the upper outer quadrant of the buttock, the anterior outer surface of the thigh, the subscapular region (Fig. 16).
When performing intramuscular injections, a syringe with a needle
Rice. 16. Areas of the body for intramuscular injections
A needle 8-10 cm long with a wide opening is placed perpendicular to the surface of the skin and a needle is inserted to a depth of 1-8 cm, pressing the skin around the puncture site with the left hand (Fig. 17). Immediately before injecting the drug, it is necessary to slightly pull back the syringe plunger to make sure that the needle does not enter a blood vessel.
7.2.1.4. Intravenous injections and infusions
|

Intravenous injections are most often performed using venipuncture (percutaneous insertion of a needle into a vein), less often - using venosection (opening the lumen of a vein). Intravenous injections are more demanding procedures than subcutaneous and intramuscular injections, and they are performed
Rice. 17. Viutrimuscular technique - usually a doctor or special injections. trained nurse,
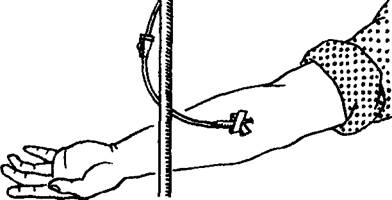
Rice. 18. Intravenous injection technique.
since the concentration of drugs in the blood after intravenous administration increases much faster than when using other methods of drug administration. Errors during intravenous injections can have the most serious consequences for the patient. For intravenous injections, the veins of the elbow, superficial veins of the forearm and hand, and sometimes the veins of the lower extremities are most often used. When performing a venipuncture, a small oilcloth pillow is placed under the elbow of the patient’s outstretched arm so that the patient’s arm is in the position of maximum extension. A tourniquet is applied above the site of the intended puncture, and with such force that only the veins are compressed, and the blood flow in the artery is preserved (Fig. 18). To increase the filling of the vein, the patient is asked to squeeze and unclench the hand several times. The skin at the injection site is thoroughly treated with alcohol. Using the fingers of your left hand, it is advisable to slightly stretch the skin of the elbow, which makes it possible to fix the vein and reduce its mobility. Venipuncture is usually performed in two stages, first piercing the skin and then the vein. With well-developed veins, puncture of the skin and vein wall can be done simultaneously. The correct placement of the needle into the vein is determined by the appearance of drops of blood from the needle. If the needle is already connected to the syringe, then to control its position it is necessary to pull the piston slightly towards you: the appearance of blood in the syringe will confirm the correct position of the needle. After this, the previously applied tourniquet is released and the medicinal substance is slowly injected into the vein.
After removing the needle and re-treating the skin with alcohol, the injection site is pressed with a sterile cotton swab or a pressure bandage is applied to it for 1-2 minutes.
|
Intravenous infusions are used to administer large quantities of different solutions (3-5 liters or more); they are the main method of so-called ////-fusion therapy. Intravenous infusions are used in cases where it is necessary to restore the volume of circulating blood, normalize the water-electrolyte balance and the acid-base state of the body.
Rice. 19. Application of the system for ma' Eliminate the phenomena of intravenous drip infusions. toxicity in severe infectious diseases, poisoning. If it is necessary to quickly administer a medicinal substance (in case of shock, collapse, severe blood loss), then jet intravenous infusions are used. If the drug must enter the bloodstream slowly, then drip administration is used. In situations where the question arises of long-term (over several days) administration of large quantities of solutions, catheterization of a vein (most often the subclavian) or venesection is used.
Intravenous infusions are carried out using a special drip system. From the point of view of compliance with the rules of asepsis and antiseptics, it is optimal to use disposable systems. Less convenient are reusable systems that require sterilization in an autoclave.
Each assembled system consists of a bottle with the drug required for infusion, a short tube with an air filter and a needle for air to enter the bottle, a dropper with a filter and two tubes, a clamp, a puncture needle, a rubber adapter tube connecting the dropper tube to the puncture needle ( Fig. 19).
Having removed the metal cap from the bottle, after wiping it with alcohol, insert a short dropper needle into it (the liquid will then flow out of the bottle through it) and a long needle of the air tube (through which air will enter the bottle). A clamp is placed on the tube in front of the dropper, the bottle is turned upside down and hung on a special stand at a height of 1 - 1.5 m above the bed. In this case, make sure that the end of the long needle (air tube) is in the bottle above the liquid level. The dropper is filled with the solution as follows: raise the tube going to the puncture needle so that the dropper (upside down) is flush with the bottle. After removing the clamp, liquid from the bottle will begin to flow into the dropper. When it is about half full, the end of the tube with the puncture needle is lowered down, and the liquid will fill this tube, displacing the air. After all the air has been forced out of the system, a clamp is applied to the tube (closer to the puncture needle). After puncturing the vein, the system is attached to the puncture needle and the desired rate of fluid flow is set using a clamp (usually 50-60 drops per minute). The infusion is stopped after the liquid stops flowing from the bottle into the dropper.
7.2.2. Complications of injections and their prevention
Various complications may arise during injections. Many of them are associated with technical errors when performing these manipulations.
A possible complication is the introduction or release of the drug into an environment other than the one in which the injection was given. Thus, the penetration of some drugs intended only for intravenous administration (for example, calcium chloride) into the subcutaneous fat layer can lead to its necrosis. On the contrary, the penetration of oil solutions during subcutaneous injections into the lumen of blood vessels is fraught with subsequent blockage of the branches of the pulmonary artery by droplets of fat (fat embolism). A similar complication (air embolism) sometimes occurs when air bubbles enter the bloodstream.
If the rules of asepsis and antisepsis are not followed due to tissue injury from blunt needles, or when too cold solutions, especially oil ones, are used, compactions (infiltrates) may develop at the injection site. In some cases, they suppurate resulting in a post-injection abscess. Trauma to blood vessels during injections can lead to hemorrhages with subsequent formation of hematomas. Such hematomas, complicated by inflammation of the vein wall and thrombosis of its lumen (phlebitis, thrombophlebitis), are sometimes observed as a result of unsuccessful puncture of the vein with a puncture of two of its walls.
Insufficient sterilization of syringes and needles, the presence of blood residues in them from a patient who has had infectious hepatitis, can lead to infection of another patient, and the disease usually manifests itself several months after the manipulation.
When performing any injections (subcutaneous, intramuscular, intravenous), the needle may break off in the tissues. This complication arises both due to defects in the needle itself and its wear and tear, and as a result of rough manipulation, accompanied by a sharp reflex muscle contraction.
A number of injection complications are associated with the direct effect of the drug itself. Due to the inattention of medical personnel, the patient may be given too large a dose of a potent drug or mistakenly given another drug. Even with the correct administration of drugs, and not only by injection, in some cases reactions develop due to the side or toxic effects of the drug.
Allergic reactions to medications are a serious problem, observed not only in patients, but also in medical personnel, especially nurses who are constantly in contact with medications.
Clinical manifestations of drug allergies are quite diverse: acute urticaria (the appearance of a blistering rash on the skin), Quincke's edema (sudden limited or diffuse swelling of the subcutaneous tissue and mucous membranes), erythema nodosum (deep damage to the blood vessels of the skin), allergic dermatitis, rhinitis, conjunctivitis, allergic damage to the digestive tract, etc.
The most serious allergic reaction that occurs during drug therapy is anaphylactic shock, which often develops suddenly and is characterized by a sharp drop in blood pressure, bronchospasm, and loss of consciousness. In the absence of timely vigorous measures, anaphylactic shock can result in the death of the patient within a few minutes. If signs of anaphylactic shock appear, it is necessary to immediately stop administering the drug (often an antibiotic), urgently administer to the patient medications that increase blood pressure (adrenaline, caffeine, etc.), antihistamines (suprastin, pipolfen), and corticosteroid hormones.
Prevention of allergic reactions when using medications should include strict consideration of the indications for their prescription, refusal (if possible) from the simultaneous use of many drugs (polypharmacy), caution when administering drug therapy to patients who have had any allergic manifestations in the past , stopping the use of the drug when the first signs of allergic reactions appear - itching, urticaria, etc.
To prevent the development of anaphylactic shock when administering immune sera, it is necessary to use the Bezredky method, which allows to avoid severe allergic reactions. When using any immune serum, first inject 0.1 ml of serum diluted 100 times subcutaneously into the flexor surface of the shoulder. After 20 minutes, the response is assessed. If the diameter of the formed tubercle does not exceed 0.9 cm and the area of hyperemia around is limited (negative reaction), then 0.1 ml of undiluted serum is administered, and then after 30-60 minutes, if there is no reaction, the rest is administered. In cases of a positive reaction, the serum continues to be administered carefully only for health reasons.
How to do subcutaneous injections correctly?
Before administering the drug, it is necessary to carry out antiseptic treatment of the hands and the bottle of medicine; you can wear gloves to ensure sterility. Next, you should adhere to the classic algorithm:
- Prepare the injection site by wiping it with a cotton ball soaked in alcohol.
- Draw the substance into the syringe, release the air from it by pressing the piston.
- With your other hand, gather the skin into a triangular fold (with the base at the bottom).
- Insert the needle at an angle of 45 degrees to 2/3 of its length (about 1-2 cm deep).
- Pressing the plunger with your free hand, smoothly push the medicine into the subcutaneous layer.
- Press the injection site with a cotton swab moistened with alcohol, remove the needle, and wash your hands.
After administration of the drug, it is recommended for 15-30 minutes. monitor your health in case of allergic reactions and complications. This is especially true for the first injection.