Successful vaccinations against viral diseases such as smallpox, polio or whooping cough are without a doubt among the greatest triumphs of modern medicine. Why, with such successes, is it not possible to create vaccines against all viruses? The development of vaccines over the past decade has not only been a success story: insufficient vaccine protection against disease, as well as the harm caused by misguided immune responses following infection by wild species in vaccinated individuals, has meant that further development of certain vaccines has been interrupted. As was said: we have “simple” vaccines. Creating protection against the disease has turned out to be much more difficult for many viruses than the successfully created vaccines suggest. Only a clear understanding of the interaction of the immune system with the relevant pathogen can help to accurately determine protective immunity, target vaccination strategies and avoid pathological immune reactions developing after vaccination.

This article aims to give the reader a better understanding of the immunological basis of vaccination against viral infections. These basics will help you better understand vaccination recommendations, the risks of vaccination and contraindications associated with it. They should also provide insight into the processes and challenges of vaccine development.
What does vaccination want to achieve?
The goal of each vaccination is to create an immunological memory so that when encountering an infection, clinical manifestations of the disease can be avoided. Immunological memory is the ability of a specific immune system to react stronger and faster during a second confrontation with the same antigen. The purpose of vaccination is also the primary activation of pathogen-specific T and B lymphocytes. The disease after infection occurs, on the one hand, as a result of the cell-damaging action of the pathogen (cytopathogenicity), and, on the other hand, as a result of an immune reaction (immunopathology). It is important to know and understand these two forms of pathogen-induced pathology and that immune responses not only protect but can also contribute significantly to disease. It follows that the goal of vaccination is not only to eliminate the pathogen as quickly as possible, but also to ensure that the immune reaction proceeds in such a way that, as little as possible, immune pathology occurs.
Creation and maintenance of immunological memory
Activation of virus-specific lymphocytes requires representation of viral structures through antigen-specific T and B cell receptors in a specific context. This “inflammatory” context is associated both with the anatomical environment (lymph nodes, germinal centers), as well as with additional signals such as soluble cytokines, or within cell-cell contacts mediated by ligand-receptor interactions. These conditions are usually met in live vaccines. When using dead vaccines, they must be created artificially. This requires the use of adjuvants, the “dirty little secret” of immunologists. Adjuvants cause local inflammatory reactions and thereby support the most effective processing and transport of viral antigens to secondary lymphatic organs.
The most important and effective mechanism for maintaining virus-specific immunity is periodic “reexposition”. These reinfections are usually asymptomatic or cause only mild symptoms and act as a natural “booster” of the immune system. Also, to a small extent, chronic or latent infections that mediate constant or intermittent stimulation of B and T cells can take on this Booster function. In this way, live vaccines in particular can leave lifelong immunity even without refreshment or reexposure. A recent study on immunity against smallpox showed detectable B- and T-cell immunity up to 75 years after vaccination, without further exogenous exposure to the pathogen.
B cell memory
Naive (virgin) B cells, upon contact with viral antigen, are activated and proliferate along the edges of the T-cell zones of the spleen or in the periarteriolar lymphatic tract (PALS) of the lymph nodes. Activated B cells then either remain in the marginal zones and differentiate into short-lived plasma cells, or move to B cell follicles and initiate a germinal center reaction there with the help of virus-specific CD4+ T cells. There they optimize their binding abilities, carry out a class change from IgM to IgG and, at the same time, differentiate into memory B cells (Fig. 1). Probably, long-living plasma cells are formed in the germinal center and then move from there to the bone marrow. They are critical antibody-producing cells and determine the level of antiviral serum antibodies. The bone marrow contains the most important survival factors, including contact with stromal cells. An important differentiation factor for long-lived plasma cells is the transcription factor Aiolos.
Memory B cells are detected within a dozen years after the first infection or vaccination. The lifespan of plasma cells in human bone marrow, however, has not been established. It is likely that redifferentiation of memory B cells into long-lived plasma cells is necessary in order to maintain a pool of these cells for a sufficiently long time. Expression of a functional B cell receptor as well as expression of the BAFF receptor are essential for B cell survival. Whether repeated contact with the viral antigen is necessary seems quite controversial. It is also possible that antigen-independent inflammatory signals, for example through the Toll-like receptor (TLR), may influence the survival of memory B cells.
T cell memory
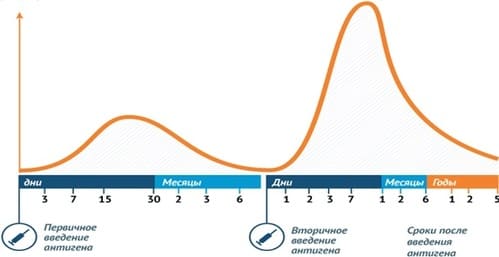
Following viral infection, there are three phases of antiviral T cell response (Figure 2). In the expansion phase, there is a strong proliferation of T cells possessing receptors for viral antigens. Brief contact with an antigen in the appropriate context is quite sufficient to cause “imprinting” of the differentiation program at the cell level, which, along with proliferation, also includes differentiation stages. At the end of the expansion phase, the maximum number and function of antiviral effector T cells is achieved. The next phase of contraction is regulated by the limited presence of antigens and cytokines as a result of virus elimination, as well as various cell death-inducing molecules, such as perforin or CD95. In this case, only a small number of cells survive, which then, at the end of the acute immune reaction, form a pool of memory cells. The preservation (maintenance) phase is characterized by the slow homeostatic proliferation of activated T cells, thereby compensating for the loss of cells associated with their limited lifespan. This homestatic proliferation requires neither antigen nor the presence of MHC molecules. The cytokine IL-7 for survival and the cytokine IL-15 for proliferation of memory T cells are important.
It is not clear whether the mere presence of virus-specific memory T cells presupposes the ability to mount a protective immune response. Due to the presence of differentiating markers, it is possible to distinguish “. The experimental model provides good indications that, above all, “effector-memory T cells,” which can circulate outside the lymphatic tissue, can also provide rapid protective T-cell immunity. These cells probably require intermittent contact with antigen to maintain their high degree of differentiation.
The vaccine should also induce long-lived plasma cells and effector-memory T cells. In order to maintain a pool of these cells for a long time, which can mediate effective vaccine protection, repeated stimulation of memory cells with persistent immunizing antigens, exogenous reinfections or Booster vaccinations is probably important.
Vaccination is important!
Vaccination (active immunoprophylaxis) is a set of measures aimed at developing anti-infectious immunity by introducing an antigen (AG) of infectious disease agents into the human body. Vaccination is recognized by WHO as an ideal method for preventing human diseases. High efficiency, ease of implementation, and the possibility of wide coverage of vaccinated individuals with the aim of mass prevention of the disease have brought active immunoprophylaxis to the level of government priorities in most countries of the world. The set of vaccination measures includes the selection of persons to be vaccinated, the choice of the vaccine preparation and the determination of the scheme for its use, as well as (if necessary) monitoring the effectiveness, stopping possible pathological reactions and complications.
Vaccines and their use:
- Active immunoprophylaxis drugs
- Live vaccines - attenuated strains of pathogens (viruses and bacteria)
- Killed vaccines are antigenic material made from killed pathogens of infectious diseases.
- Genetically engineered vaccines are antigenic material of pathogens obtained using genetic engineering methods; contains only highly immunogenic components that contribute to the formation of protective immunity
- Chemical vaccines - vaccines obtained by chemical treatment of the complete antigenic complex of pathogens
- Anatoxins are antigenic materials of toxins of infectious disease agents that lack toxic properties.
- Various combinations of vaccines and toxoids in one drug (associated vaccines) are used to create immunity against several infections simultaneously.
Vaccines are introduced into the body:
- Parenteral (intramuscular, subcutaneous, intradermal and cutaneous [scarification])
- Inside (per os)
- Application to the nasal mucosa.
- Most vaccines can be used for emergency post-exposure prophylaxis of infectious diseases (prevention of disease in persons in contact with the patient).
- When a vaccine is introduced into the body, a reaction develops. It includes both the formation of protective immunity and a number of somatic manifestations, often recorded in the post-vaccination period
- A short-term increase in body temperature to subferile values, short-term malaise, slight hyperemia at the site of injection of the drug; regarded as a possible (conditionally normal) reaction to vaccination
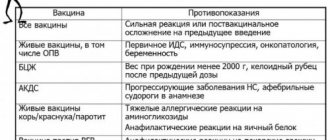
- Severe vascular, neurological changes, anaphylactic shock (always considered as a pathology of the post-vaccination period) are a contraindication for subsequent vaccination with this drug.
History The widespread spread of infectious diseases at all times not only led to the death of many millions of people, but was also the main reason for short human life expectancy. Since E. Jenner made the first smallpox vaccinations 219 years ago, there has been no more effective way in the world to prevent infectious diseases than preventive vaccinations, otherwise called vaccination (immunization). Immediately after birth, a person comes into contact with a huge number of microorganisms. To resist them, the body “turns on” the mechanisms of natural immunity, which begins to form in the womb and is established in the first years of life. Some microorganisms cannot overcome this barrier and are therefore not dangerous to a healthy body. Another part of microorganisms cannot be stopped by this barrier and, penetrating into the human body, causes disease and begins a battle with the body. The outcome of this battle cannot always be predicted... If the body nevertheless turns out to be stronger than the virus or microbe, then the disease will be suppressed, and the body will receive information about ways to combat them - specific (acquired) immunity. True, in the very first contraction, serious damage can be caused to the body - complications that sometimes remain for the rest of your life. When you encounter the virus again, the acquired immunity will already have information about methods of combating it and will be able to protect the body without much effort. The meaning of vaccination is that vaccines are introduced into the human body - weakened or killed pathogens of various infections (or artificially synthesized proteins that are identical to the proteins of the pathogen). All vaccine prevention is based on the existence of the phenomenon of immunological memory. Thanks to it, it is possible to artificially form long-term, sometimes lifelong, anti-infectious immunity. Immunological memory is the body’s ability to give an accelerated immunological reaction to repeated introduction of an antigen. After the vaccine is administered, protective specific antibodies (immunoglobulins) appear. They are not detected immediately, but only on days 5-7, then their number quickly increases by days 10-12, and maximum by days 20-22. Then the number of specific antibodies decreases and after a few months is not detected at all or is detected in low titers. But the immunological memory remains, its carriers are small T- and B-lymphocytes, specifically rearranged during the primary response. If the pathogen penetrates a second time, then antibodies appear much faster - after 1-2 days - and in greater quantities than with the primary response.
Immunological memory
Some vaccines create immunity the first time, while others have to be given repeatedly. The so-called revaccination is an event aimed at maintaining the immunity developed by previous vaccinations. A weakened pathogen (obtained from weakened or killed microorganisms, their metabolic products, or from their antigens obtained by genetic engineering or chemical means), entering the human body, causes a response from the body to fight the virus. As a result of this fight, the body produces antibodies to the virus, thus gaining experience in effectively neutralizing the virus (acquired immunity). It is this experience that will subsequently be used when encountering a similar real pathogen - antibodies will stop the development of the disease at the very beginning of the disease or, if infection does occur, will allow the body to cope with the virus without serious complications. Thus, a vaccine is a training test for the body to fight a particular type of infection.
Schematic representation of how the immune system works
Thus, vaccines target a person's natural response to disease to stimulate the immune system so that when encountering a specific pathogen in the future, the immune system can “remember it” and respond appropriately, stopping the progression of the disease or reducing its severity. Specific immunity is initiated by vaccination. Vaccines stimulate the immune system to the same extent as the infectious agent itself and can potentially provide more effective protection against certain pathogens. Most importantly, the protection provided by vaccination helps to avoid the development of complications associated with the course of such a disease. The benefits of vaccination far exceed this for the development of vaccine-preventable diseases.
Vaccination achievements Today, mass vaccination is a factor in economic growth on a global scale. Vaccination programs around the world save 6 million lives every year—children's lives. 750 thousand children do not become disabled. Vaccination gives humanity 400 million extra years of life every year. And every 10 years of life saved provides 1% of economic growth. Vaccination is recognized as the most effective medical intervention invented by man. Comparable results were achieved only by using clean drinking water.
Immunoprophylaxis is listed first on the list of the 10 greatest health achievements of the 20th century

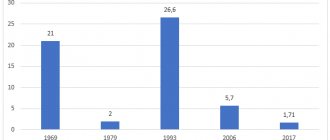
Smallpox Achievement: Smallpox is the only infectious disease completely eradicated by humanity. It is not known exactly when this deadly disease began its march across the planet, but it is known that it swept across China in the 4th century, and in the middle of the 6th century it struck Korea. In 737, smallpox killed more than 30% of Japan's population (the mortality rate in densely populated areas reached 70%). In the 15th century, Europe was already a complete smallpox hospital. In the 17th-18th centuries in Europe, an average of about 10 million people suffered from smallpox every year, of whom about 1.5 million died. During large smallpox epidemics, the mortality rate reached 25-40%. In 1796, the English doctor E. Jenner decided on a revolutionary experiment for those times: on May 14, in the presence of doctors and the public, he removed smallpox from the hand of a young milkmaid who had accidentally contracted cowpox, and inoculated it into an eight-year-old boy. Smallpox took hold, developed only in two grafted areas and proceeded normally. Then, on July 1, Jenner inoculated the boy with natural human smallpox, which, as he was protected by a protective vaccination, did not take hold. From this moment the history of vaccination begins, as well as the destruction of smallpox on the planet. Cowpox vaccinations began to be practiced in many countries, and the term “vaccine” was introduced by Louis Pasteur, from the Latin vacca, “cow.” Smallpox persisted for almost two hundred years after the invention of vaccination. In the 20th century, the virus claimed the lives of 300-500 million people. In the late 1960s, smallpox affected 10-15 million unvaccinated people. In 1958, Deputy Minister of Health of the USSR V. M. Zhdanov spoke at the XI session of the World Health Assembly with a program to eradicate smallpox throughout the world. The speech was followed by a resolution adopted by the assembly and marking the beginning of the campaign to combat smallpox. In 1967, WHO decides to intensify the eradication of smallpox through mass vaccination of humanity. The last case of natural smallpox infection was described in Somalia in 1977. The eradication of smallpox from the planet was officially announced in 1980 at the WHO Assembly. Today, viruses are contained in only two laboratories: in Russia and the USA.
Rabies Achievement: A disease that was 100% fatal was defeated with a vaccine. In 1885, Louis Pasteur developed a vaccine against rabies, a disease that in 100% of cases resulted in the death of the patient and terrified people. It came to the point of demonstrations under the windows of Pasteur’s laboratory demanding that experiments on the invention of an “antidote” be stopped. Pasteur hesitated for a long time to try the vaccine on people, but chance helped. On July 6, 1885, a 9-year-old boy was brought into his laboratory, who was so bitten that no one believed in recovery. Pasteur's method was the last hope for salvation. The boy fully recovered, which brought Pasteur truly worldwide fame. Today, the principle of vaccination against this disease is not very different from that which was used in the first vaccination experience. Immediate wound cleansing and immunization given within a few hours of contact with a suspected rabid animal can prevent the development of rabies and death. Every year, more than 15 million people worldwide receive post-exposure vaccination to prevent the development of rabies; this is estimated to prevent hundreds of thousands of deaths each year.
Tuberculosis Achievement: WHO adopted a program to combat tuberculosis. Between 1990 and 2013, mortality from tuberculosis decreased by 45%. Robert Koch was able to isolate the bacterium that causes tuberculosis in 1882. But it was not until 1921, when a live bacterial vaccine (BCG) was developed at the Pasteur Institute, that tuberculosis ceased to be considered a deadly disease. Nowadays, the BCG vaccine is the main drug for the specific prevention of tuberculosis, recognized and used throughout the world. Attempts to prepare an anti-tuberculosis vaccine from other weakened strains or individual fractions of microbial cells have not yet yielded significant practical results. About 2 billion people, almost a third of the world's population, are infected with tuberculosis bacteria. The risk that infected people will develop TB in their lifetime is 10%. Vaccination against tuberculosis is an integral part of the calendars of many countries (mandatory in more than 60 countries of the world, and officially recommended in another 118). Between 1990 and 2013, mortality from tuberculosis decreased by 45%. An estimated 37 million lives were saved from 2000 to 2013 by preventing and treating tuberculosis.
Polio Achievement: 99% of the way to eradicating polio worldwide has been achieved. There was a time when polio was feared throughout the world as a disease that struck suddenly and caused lifelong paralysis, mainly among children. On April 12, 1955, a large-scale study was successfully completed in the United States, confirming the effectiveness of the Jonas Salk vaccine, the first vaccine against polio. The importance of this event cannot be overestimated. In 1954, there were more than 38,000 cases of polio in the United States, and after 10 years of the Salk vaccine, in 1965, the number of polio cases in the United States was only 61. In 1988, governments created the Global Polio Eradication Initiative (GPEI). ), to rid humanity of this disease forever. In 1988, when the GPEI was created, the disease was causing paralysis in more than 350,000 people each year. Since then, the number of polio cases has decreased by more than 99% (only 406 cases were reported in 2013). In fact, this is the largest peacetime mobilization of people in history. Today, there are two types of vaccines available to prevent polio—oral polio vaccine (OPV) and inactivated polio vaccine (IPV). OPV or oral vaccine can be administered by anyone, even volunteers. Unlike most diseases, polio can be completely eradicated. There are three strains of wild poliovirus, none of which can survive for long periods of time outside the human body. In 2014, only three countries in the world (Afghanistan, Nigeria and Pakistan) remain polio-endemic, down from more than 125 in 1988. Currently, 80% of the world's population lives in certified polio-free regions. The world can be freed from the threat of polio if there is universal commitment to vaccination - from parents to government workers and from political leaders to the international community.
Diphtheria Achievement: as a result of immunoprophylaxis, the incidence of diphtheria has sharply decreased; it has been eliminated in many countries. Already in the first century AD one can find mention of diphtheria, then called “strangulated loop” or “deadly ulcer of the pharynx.” Until the beginning of the 20th century, diphtheria claimed thousands of children's lives every year, and medicine was powerless to alleviate their suffering and save them from severe agony. On December 26, 1891, Emil von Behring saved the life of a sick child by giving him the first diphtheria vaccination. The success of the experiment was impressive, many children were saved, but still this victory was only partial, and the Bering serum did not become a reliable remedy that saved all children. And then Bering was helped by his colleague and friend Paul Ehrlich: he managed to establish large-scale production of the serum, calculate the correct dosages of the antitoxin and increase the effectiveness of the vaccine. In 1894, the improved serum was successfully tested on 220 sick children. For saving children in 1901, Behring was awarded the first Nobel Prize in Physiology or Medicine “for his work on serum therapy, mainly for its use in the treatment of diphtheria, which opened new paths in medical science and gave doctors a victorious weapon against the disease and of death". The prophylactic serum, which is now used against diphtheria, was discovered by Dr. Gaston Ramon, an employee of the Pasteur Institute in Paris. During the period 1980-2000. The total number of reported cases of diphtheria has been reduced by more than 90%. Introduction in 1994 of mass immunization of the Russian population against diphtheria with repeated revaccination of adults in 2003-2004. made it possible to provide sufficient specific protection of the population from this infection. This led to a decrease in the incidence of diphtheria in Russia from 26.8 in 1994 to 0.01 per 100 thousand population in 2009-2011. The World Health Organization recommends vaccination for all countries of the world without exception.
Human papillomavirus Advances: Vaccines have been developed to prevent infection with the oncogenic viruses HPV-16 and HPV-18, which cause cervical cancer. Back in 1976, a hypothesis was put forward about the relationship between human papillomaviruses (HPV) and cervical cancer. In the mid-seventies, scientist Harald zur Hausen discovered that women with cervical cancer were invariably infected with HPV. At that time, many experts believed that cervical cancer was caused by the herpes simplex virus, but Harald zur Hausen found not herpes viruses, but papilloma viruses in cancer cells, and suggested that the development of cancer occurs as a result of infection with the papilloma virus. Subsequently, he and his colleagues were able to confirm this hypothesis and establish that most cases of cervical cancer are caused by one of two types of these viruses: HPV-16 and HPV-18. Harald zur Hausen's research in the field of HPV infection formed the basis for understanding the mechanisms of carcinogenesis induced by the papilloma virus. Vaccines have subsequently been developed that can prevent infection by the HPV-16 and HPV-18 viruses. This treatment will reduce the amount of surgery required and overall reduce the threat posed by cervical cancer. After a full course of vaccination, protective antibodies are detected in more than 99% of vaccinated people. Modern mathematical models show that when girls aged 12-13 years are covered with a full course of primary immunization (3 doses) with a vaccine against human papillomavirus infection, it is possible to predict a reduction in the risk of developing cervical cancer by 63%, and cervical intraepithelial neoplasia of the third severity (precancer) by 51%. , cytological disorders in age cohorts under 30 years old - by 27%. By the end of 2013, the human papillomavirus vaccine had been introduced in 55 countries.
Hepatitis Advances: A vaccine against hepatitis B has been available since 1982. This vaccine is 95% effective in preventing the infection and its chronic consequences and is the first vaccine against one of the major human cancers. There are five hepatitis viruses, defined as types A, B, C, D and E. Types B and C are of particular concern because most people infected with these viruses may not experience any symptoms early in the disease and become aware that are infected only when the infection becomes chronic. Sometimes this can be decades after infection. In addition, these two viruses are the leading cause of cirrhosis and liver cancer, causing nearly 80% of all liver cancer deaths. The first hepatitis B vaccine became available in China. They began using a vaccine prepared from blood plasma obtained from donors from among patients who had a long-term infection with the hepatitis B virus. In 1987, the plasma vaccine was replaced by the next generation of the vaccine against the hepatitis B virus, which used the technology of genetic modification of recombinant DNA in the cells of a yeast microorganism. It is sometimes called a genetically engineered vaccine. Both types of vaccines are safe and highly effective. More than 240 million people have chronic (long-term) liver infections. About 780,000 people die each year from the acute or chronic effects of hepatitis B. After a full series of vaccinations, more than 95% of infants, children of other age groups and young adults develop protective levels of antibodies. Protection lasts for at least 20 years and possibly a lifetime. In many countries where typically 8% to 15% of children had chronic hepatitis B virus infection, vaccination has reduced rates of chronic infection among immunized children to less than 1%.
Haemophilus influenzae Achievements: Haemophilus influenzae vaccination is available in 189 countries, significantly reducing the incidence of meningitis and bacteremia caused by Haemophilus influenzae. Haemophilus influenzae infection remains a serious threat to life and health, causing, according to experts, about 3 million cases of severe illness in the world and more than 350 thousand deaths per year. Almost all victims are children under the age of five, with children aged 4 to 18 months most vulnerable to infection. By the end of 2013, the Hib vaccine had been introduced in 189 countries. Current Hib vaccines are very effective. The incidence of all forms of infection in developed countries where routine immunization is carried out has decreased by 85-98%. Numerous trials of polysaccharide vaccines have been conducted in Europe and North America. In particular, a clinical trial in the UK (1991-1993) showed an 87% reduction in the incidence of haemophilus influenzae meningitis. In Holland, during a similar study, a complete absence of cases of meningitis of hemophilic etiology was recorded within 2 years after the start of immunization.
Measles Achievement: Between 2000 and 2013, measles vaccination resulted in a 75% reduction in global measles deaths. Back in the mid-20th century, measles was considered a “mandatory” disease that every child should have. In the mid-1960s, an effective vaccine against measles was finally developed in the former Soviet Union. At the same time, the American scientist John Enders made his discovery of a vaccine against measles. But before vaccines were widely used, measles continued to claim children's lives. In 1980, before widespread vaccination, there were an estimated 2.6 million deaths from measles. Measles is a leading cause of death among young children, even with the availability of a safe vaccine. Between 2000 and 2013, measles vaccination led to a 75% reduction in global measles deaths. In 2000-2013 Measles vaccination has prevented an estimated 15.6 million deaths, making measles vaccine one of the most significant public health advances. It is planned that in 2015, mortality from measles will be reduced by 95% (20 times) compared to 2000, and by 2021, measles (as well as rubella) will be completely eliminated in at least five WHO regions.
Pneumococcal infection Achievements: mass vaccination reduces the incidence of pneumococcal meningitis and severe pneumonia in children by more than 80% and the incidence of all pneumonia and otitis by more than a third. Pneumococcus was identified quite a long time ago - in 1881. But vaccines began to be developed only in the second half of the 20th century. The difficulty in creating such vaccines was (and is) the huge number of types of pneumococcus. Before widespread immunization with the 7-valent pneumococcal conjugate vaccine, the average annual incidence among children <2 years of age was 44.4/100,000 in Europe and 167/100,000 in the United States. The World Health Organization projects that global use of pneumococcal vaccination will prevent 5.4-7.7 million child deaths by 2030.
Whooping cough Achievements: As a result of large-scale vaccination carried out in the 1950-1960s in industrialized countries, there was a sharp reduction in the incidence (by more than 90%) and mortality from whooping cough. It was only in 1906 that scientists Jules Berdet and Octave Zhangou, working at the Pasteur Institute in Brussels, isolated the whooping cough bacillus. But even after this, doctors did not have more funds to treat whooping cough infection. They appeared only during the Second World War. The first pertussis vaccine appeared in the USA in 1941, and the first combined DPT vaccines were introduced into vaccination practice abroad in the late 40s of the 20th century. The greatest number of whooping cough diseases occurs between the ages of 1 and 5 years. The incidence of whooping cough in the past was almost universal and was second only to measles. In 2008, approximately 82% of all infants worldwide were vaccinated with three doses of pertussis vaccine. WHO estimates that approximately 687,000 deaths were prevented by pertussis vaccination in 2008. The main goal of whooping cough vaccination is to reduce the risk of severe infection in infants. The global priority is to achieve 90% coverage among infants with three doses of high-quality pertussis vaccine, especially where the disease poses a major health threat to infants and young children.
Rubella Achievements: Thanks to large-scale rubella vaccination over the past decade, rubella and congenital rubella syndrome (CRS) have been virtually eliminated in many developed and some developing countries. There have been no endemic (naturally transmitted) cases of rubella infection in the WHO Region of the Americas since 2009. The causative agent of rubella in 1961 was almost simultaneously isolated by several scientists: P. D. Parkman, T. X. Weller and F. A. Neva. But even earlier, in 1941, the Austrian researcher N. Gregg described various fetal anomalies in connection with its intrauterine infection with the rubella virus during the illness of the pregnant mother. Vaccinations can significantly reduce fetal deaths in pregnant women and the risk of congenital rubella syndrome (CRS), which causes birth defects. In Russia, which began mass vaccination against rubella only in 2002-2003, great success has been achieved: in 2012, the incidence dropped to 0.67 per 100 thousand. Among patients with rubella, unvaccinated persons and persons with an unknown vaccination history predominated (their share in 2012 was 90.7%), so that conditions were created for the implementation of a rubella elimination program and the prevention of congenital rubella syndrome (CRS).
Mumps (mumps) Advances: In countries with widespread immunization against mumps, the incidence has declined significantly. The disease was described by Hippocrates, but only in 1934 was the viral nature of the pathogen proven. Until the 1960s, when vaccines became available, mumps was a widespread disease in all parts of the world. Every year, from 100 to 1000 people per 100 thousand people fell ill. Although the disease is mild, it can be dangerous due to complications - meningitis, sensorineural deafness, orchitis (in boys). By the end of 2013, mumps vaccine had been introduced nationally in 120 countries. In 2006, Russia recorded the lowest incidence rate of mumps in the entire history of observation - 1.64 per 100 thousand population. Compared to 1981, the incidence decreased by 294 times. The incidence of mumps has been steadily declining over the past five years, which was a consequence of the high level of vaccination coverage among children (and especially revaccination) - from 72% in 1999 to 96.5% in 2006. At the end of 2013, the incidence rate in our country was 0.2 per 100 thousand people.
Meningococcal infection Achievements: vaccination can prevent the development of such a deadly disease as meningococcal meningitis. The highest rates of the disease are found in the meningitis belt of sub-Saharan Africa, stretching from Senegal in the west to Ethiopia in the east. Before 2010 and mass vaccination campaigns, it was estimated that 80-85% of all cases in the meningitis belt were caused by group A meningococcus.
At the same time, epidemics occurred every 7-14 years. Since then, the proportion of serogroup A has declined sharply. In December 2010, a new meningococcal group A conjugate vaccine was introduced throughout Burkina Faso and parts of Mali and Niger, where a total of 20 million people aged 1–29 years were vaccinated. Subsequently, in 2011, these countries reported the lowest ever number of confirmed cases of meningitis A during the epidemic season. Vaccination is carried out once, the effectiveness is about 90%, immunity is formed on average within 5 days and lasts 3-5 years.
Influenza Achievements: the use of influenza vaccination reduces the incidence rate by 1.4-1.7 times, helps reduce the severity of the disease, and prevents the development of severe complications and deaths. Influenza means “to catch” in French. An epidemic of a flu-like disease was first described in 412 BC. Hippocrates. The first pandemic (global epidemic) of influenza, which claimed many lives, was recorded in 1580. And since then, this disease has continued to sweep the planet. During the famous Spanish Flu epidemic in 1918, 20-40 million (or more) human lives were lost. Safe and effective vaccines against this disease have been available and used for over 60 years. The composition of vaccines changes every year. This is done to provide maximum protection against the “wild” influenza virus. Immunity after administration of the vaccine is formed within 14 days and lasts throughout the season.
Tetanus Achievement: By the end of 2013, a vaccine to prevent maternal and neonatal tetanus had been introduced in 103 countries. As a result of immunization, an estimated 82% of newborn children were protected. The mortality rate for tetanus is very high (higher only for rabies and pneumonic plague). In regions where there are no preventive vaccinations and qualified medical care, the mortality rate is about 80%. But this infection can be prevented with preventive vaccinations. In 1923, the French immunologist G. Ramon obtained tetanus toxoid, which was used to prevent the disease. The introduction of tetanus vaccination in the United States in the 1940s caused the overall incidence of the disease to decline from 0.4 per 100,000 population in 1947 to 0.02 per 100,000 population in the late 1990s. In a double-blind, controlled study conducted in rural Colombia, neonatal tetanus did not occur in infants born to mothers who received two or three doses of the vaccine. While in the unvaccinated control group of newborns, the mortality rate was 78 deaths per 1000 live births. The effectiveness and efficiency of tetanus toxoids have been documented. In most clinical trials, effectiveness ranged from 80% to 100%. Today, maternal and neonatal tetanus remains a public health problem in 25 countries, predominantly in Africa and Asia, where vaccination coverage is low.
Cholera Advances: There are two types of safe and effective oral cholera vaccines that have been used successfully in vulnerable populations living in high-risk areas. In the 19th century, cholera spread from its original reservoir in the Ganges River Delta in India throughout the world. Six consecutive pandemics have killed millions of people on every continent. This “disease of unwashed hands” terrified people for a long time and led to cholera riots, when patients burned down hospitals, suspecting that doctors were “poisoning” them. Today, cholera affects 3–5 million people each year, and 100,000–120,000 deaths from the disease occur. There are currently two types of safe and effective oral vaccines on the market that can prevent the spread of epidemics. Both types are whole cell killed vaccines, one of which contains a recombinant B subunit. Both vaccines provide sustained protection of more than 50% over two years in endemic areas. Both types of vaccines have been pre-evaluated by WHO and are licensed in more than 60 countries.
References: 1. Aleksandrova V.A. Basics of the immune system of the gastrointestinal tract. Methodological manual.-SPb.-2006.-43p. 2. Vodeyko L.P. The effectiveness of the use of antioxidants in complex therapy of influenza. Abstract of thesis….candidate of medical sciences. St. Petersburg, 2000.- 22 p. 3. Grinevich V.B. and others. Clinical aspects of diagnosis and treatment of intestinal dysbiosis in general therapeutic practice (educational manual). St. Petersburg, 2003.- 37 p. 4. Avian influenza: the origin of infectious biodisasters. /ed. acad. V.I. Pokrovsky. St. Petersburg, 2005.-269 p. 5. Desheva Yu.A. Ways to improve the live influenza vaccine and tactics for its use in preparation for a pandemic. Abstract thesis...doctor of medical sciences. St. Petersburg 2009.- 40 p. 6. Dondurei E.A. Etiology and clinical and laboratory characteristics of acute viral infections with combined damage to the respiratory and gastrointestinal tracts in children. Abstract of thesis….candidate of medical sciences. St. Petersburg 2007.-24s. 7. Drinevsky V.P., Osidak L.V., Gordeev V.I. and others. Standardized principles of diagnosis, treatment and emergency prevention of influenza and other acute respiratory infections in children. St. Petersburg, 2004.-96p. 8. Zuev V.A. "Slow viral infections of humans and animals." M.: Medicine. 1988. - 250 p. 9. Ershov F.I., Kiselev O.I. Interferons and their inducers (from molecules to drugs). M.: GEOTAR-Media. 2005.-356p. 10. Ershov F. I. Antiviral drugs. Handbook (2nd edition). M.: GEOTAR-Media. 2006.-311p. 11. Isakov V.A., Kovalenko A.L., Turkin V.V., Aspel Yu.V. The use of new immunotropic and antioxidant agents in the treatment of influenza and acute respiratory infections. Guide for doctors. St. Petersburg-V.Novgorod. 2000. - 74 p. 12. Kolobukhina L.V., Merkulova L.N., Burtseva E.I., Shchelkanov M.Yu. Oseltamivir (Tamiflu): the possibility of highly effective treatment of influenza. //Russian medical journal. 2008.-T.16.-P.69-73. 13. Lobzin Yu.V., Zakharov V.I. Rehabilitation and clinical examination of infectious patients. Hippocrates, St. Petersburg, 1994.-214 p. 14. Maleev V.V. Problems of infectious pathology at the present stage. //Epidem. and infectious diseases.2006.-No.4.-P.11-14. 15. https://diseases.academic.ru/202/ 16. https://ru.wikipedia.org/wiki/ 17. https://www.yaprivit.ru/vaccination/vaccination-achivement/
What is ideal vaccine immunity?
Typical humanopathogenic viruses have evolved through a process of long-term coevolution with their host. The result of this joint development appears to be optimal adaptation to each other. The ideal virus-host relationship is determined by the principle of “balanced pathogenicity”: infection ideally causes as much damage as is necessary to maintain the life cycle of the pathogen. On the host side, the immune system is a complex result of constant interaction with many different microbial pathogens. Each virus, in its evolving context, has formed slightly different elements of the immune system, limited in its defense. The formation of specific memory reactions allows the disease to be prevented after repeated infection.
Based on these ideas, ideal vaccine immunity should be as similar as possible to that of evolutionarily optimized immunity after wild infections. This will most likely ensure that immunity occurs in place, at a reasonable rate, and with appropriate interaction between T and B immune cells. Ideally, the vaccine would imitate the important parameters of a wild infection, which include:
- entrance gate,
- typical inoculation dose,
- tropism for cells
- replication dynamics and
- ability to persist
As the examples show, a vaccine against measles, rubella, polio, chickenpox or hepatitis B, a good vaccine does not necessarily have to follow the natural path of infection, nor replicate in the host. This applies, however, to many other viruses, not to the same extent. The development of vaccines against HIV, HCV, CMV, EBV, HSV, rotavirus, RSV and other respiratory viruses is associated with significantly greater difficulties (Table 1). They can probably be resolved by taking into account the above principles. The example of RSV vaccine development illustrates this problem.
Misdirected immunity during vaccination - an example of RSV-lot100
In the early 1960s, the first RSV vaccine was created and tested on infants and young children. To do this, the virus was inactivated with formalin and an aluminum-based adjuvant was added, and the vaccine was administered to children aged 1 to 7 years in two or three intramuscular doses with an interval of 1-3 months. The vaccine was not only able to provide protection against disease following wild-type RSV infection, but also induced an exaggerated pathological response to wild-type RSV infection in vaccinated children. Many children were hospitalized with diseases of the lower respiratory tract. In one study, the rate of RSV-related hospitalization in vaccine recipients was exactly 80%, compared with 5% in controls. Tragically, two vaccinated children died from RSV infection.
A good immune response to a vaccine is usually determined by measuring antibodies. The majority of children vaccinated with RSV-lot100 seroconverted after vaccination with high titers against RSV-F protein. The problem with the vaccine was thus not the lack of induction of immunity, but the induction of “wrong” “false” immunity. To understand and avoid such pathological immune reactions, it is necessary to have a clear understanding of the role of specific B and T cell responses in the control of viral infections and immunologically mediated pathology. In particular, the following questions should be answered:
- What role does B cell play? T-cell immunity in protection against disease?
- What role do CD4+- vs. CD8+ T-cells, what role do Th1- vs. Th2 cells?
- What is the role of local vs. systemic T-cell immunity, virus-specific IgA vs. IgG?
Some of these immunological aspects will be presented below. Ultimately, they were studied individually for each virus, since each virus-host interaction is different from each other. These considerations can best be illustrated with a specific example. For this purpose and in further presentation, we must use RSV infection.
What to do if a child has a reaction to a vaccine?
If a reaction occurs, parents should call the facility where they received the vaccine and tell them about it. Ideally, healthcare workers should call themselves within the first or second day and find out whether the child has a reaction to the vaccine. But if there is no call, the parents need to call themselves, since the doctor in any case should know how the child survived the vaccination.
Wherever a child is vaccinated (by law, each of us has the right to choose a medical institution where he will be vaccinated), he will in no case be deprived of free medical care. And if a child needs medical help, it is enough to call a pediatrician at your place of residence. However, before calling an ambulance or a pediatrician to your home, it is recommended to call and discuss the situation with the doctor who administered the vaccination. There are cases when a completely standard situation is seen by parents as threatening the life of the child. In this case, the doctor will reassure the parents and give the necessary recommendations.
How do antibodies convey antiviral immunity?
Antibodies are soluble substances secreted by B cells. They circulate in the plasma and can reach mucosal surfaces via transcytosis. Dense tissues are not accessible to antibodies. The most important antiviral effector function is extracellular neutralization (Fig. 3). In this case, the surface proteins of the virus, which are especially necessary for entry into the cell, are bound and masked, so that infection of the target cell is prevented. Antibody binding is a prerequisite for two other effector mechanisms, complement-mediated virolysis, and Fc-mediated phagocytosis of viruses. If this does not happen, then the effectiveness of antibody-mediated immunity is limited. Although antibodies can theoretically bind, as part of viral maturation, viral proteins embedded in the cell membrane and mediate cell lysis through antibody-dependent cytotoxicity (ADCC), the significance of this mechanism in vivo remains controversial. Also, the significance of intracellular neutralization of viruses by antibodies has not been established. Antibodies always appear quickly and can recognize free viruses and prevent cell infection. Once an infection of the cells has occurred, they remain inactive and cannot provide any sterilizing immunity.
The quality of antiviral antibody responses can best be understood by testing their ability to neutralize. Unlike the commonly used ELISA method, which solely determines the binding of the antibody to viral proteins (often regardless of whether the surface or internal proteins are involved), the neutralization test measures the biological function of antibodies. It is tested whether the antibodies are actually able to prevent infection of the cell.
Characteristics of vaccines
1.Vaccine classification
2.Live vaccines
3.Killed vaccines
4.Combination vaccines
1 . Based on their purpose, vaccines are divided into preventive and therapeutic.
Based on the nature of the microorganisms from which they are created, wakiins are:
• bacterial;
• viral;
• rickettsial.
There are mono-
and
polyvaccines -
prepared respectively from one or more pathogens.
according to the method of preparation :
• alive;
• killed;
• combined.
To increase immunogenicity to vaccines
sometimes various types
of adjuvants
(aluminum-potassium alum, aluminum hydroxide or phosphate, oil emulsion), creating a depot of antigens or stimulating phagocytosis and thus increasing the foreignness of the antigen for the recipient.
2. Live vaccines
contain
live attenuated strains of pathogens with sharply reduced virulence
or
strains of microorganisms that are non-pathogenic to humans and closely related to the pathogen in antigen terms (divergent strains).
These include recombinant
(genetically engineered) vaccines containing vector strains of non-pathogenic bacteria/viruses (genes responsible for the synthesis of protective antigens of certain pathogens have been introduced into them using genetic engineering methods).
Examples of genetically engineered vaccines include the hepatitis B vaccine, Engerix B, and the rubella measles vaccine, Recombivax NV.
Since live vaccines
contain strains of pathogenic microorganisms with sharply reduced virulence, then, in essence, they
reproduce in the human body a mild infection,
but not an infectious disease, during which the same defense mechanisms are formed and activated as during the development of post-infectious immunity.
In this regard, live vaccines, as a rule, create quite intense and long-lasting immunity.
On the other hand, for the same reason, the use of live vaccines against the background of immunodeficiency states (especially in children) can cause severe infectious complications.
For example, a disease defined by clinicians as BCGitis after administration of the BCG vaccine.
Live vakiins are used for the prevention of:
• tuberculosis;
• especially dangerous infections (plague, anthrax, tularemia, brucellosis);
• influenza, measles, rabies (anti-rabies);
• mumps, smallpox, polio (Seibin-Smorodintsev-Chumakov vaccine);
• yellow fever, rubella measles;
• Q fever.
An interval of at least 1 month is recommended between administrations of live vaccines, otherwise severe adverse reactions are possible and the immune response may be reduced.
3. Killed vaccines contain killed pathogen cultures
(whole cell, whole virion). They are prepared from microorganisms inactivated by heating (heated), ultraviolet rays, chemical substances (formalin - formol, phenol - carbolic, alcohol - alcohol, etc.) under conditions that exclude denaturation of antigens.
The immunogenicity of killed vaccines is lower than that of live ones. Therefore, the immunity they evoke is short-lived and relatively less intense. Killed vakiins are used for the prevention of:
• whooping cough, leptospirosis,
• typhoid fever, paratyphoid A and B,
• cholera, tick-borne encephalitis,
• polio (Salk vaccine),
hepatitis A.
To killed vaccines
Also include
chemical vaccines
containing certain chemical components of pathogens that are immunogenic (subcellular, subvirion).
Since they contain only individual components of bacterial cells or virions that are directly immunogenic, chemical vaccines are less reactogenic and can be used even in preschool children.
Anti-idiotypic drugs are also known
vaccines that are also classified as killed vaccines. These are antibodies to one or another idiotype of human antibodies (anti-antibodies). Their active center is similar to the determinant group of the antigen that caused the formation of the corresponding idiotype.
4. Combined vaccines include artificial vaccines.
They are preparations consisting of a microbial antigenic component
(usually isolated and purified or artificially synthesized antigen of the pathogen) and
synthetic polyions
(polyacrylic acid, etc.) - powerful stimulators of the immune response.
They differ from chemically killed vaccines in the content of these substances. The first such domestic vaccine is the influenza polymer-subunit vaccine (“Grippol”),
developed at the Institute of Immunology, has already been introduced into Russian healthcare practice.
For specific prevention of infectious diseases whose pathogens produce exotoxin, toxoids are used.
Anatoxin -
it is an exotoxin, devoid of toxic properties, but retaining antigenic properties.
Unlike vaccines, when used in humans, antimicrobial immunity
antitoxic immunity
antitoxins.
Currently used:
• diphtheria;
• tetanus;
• botulinum;
• staphylococcal toxoids;
• Cholerogen-anatoxin.
Vaccines containing bacterial antigens and toxoids are called associated vaccines. Examples of associated vaccines are
— DTP vaccine
(adsorbed pertussis-diphtheria-tetanus vaccine), in which the pertussis component is represented by killed pertussis vaccine, and diphtheria and tetanus - by the corresponding toxoids;
— TAVTe vaccine,
containing O-antigens of typhoid, paratyphoid A- and B-bacteria and tetanus toxoid;
typhoid chemical vaccine
with sextaanatoxin (a mixture of toxoids of Clostridium botulism types A, B, E, Clostridium tetanus, Clostridium perfringens type A and edematiens - the last 2 microorganisms are the most common causative agents of gas gangrene), etc.
At the same time, DPT (diphtheria-tetanus toxoid), often used instead of DTP when vaccinating children, is simply a combination drug and not an associated vaccine, since it contains only toxoids.
1
.
Based on their purpose,
vaccines are divided into preventive and therapeutic.
According to the nature of the microorganisms from which they are created,
There are types of wakiins:
• bacterial;
• viral;
• rickettsial.
There are mono-
and
polyvaccines -
prepared respectively from one or more pathogens.
By cooking method
vaccines are distinguished:
• alive;
• killed;
• combined.
To increase immunogenicity to vaccines
sometimes various types
of adjuvants
(aluminum-potassium alum, aluminum hydroxide or phosphate, oil emulsion), creating a depot of antigens or stimulating phagocytosis and thus increasing the foreignness of the antigen for the recipient.
2.
Live vaccines
contain
live attenuated strains of pathogens with sharply reduced virulence
or
strains of microorganisms that are non-pathogenic to humans and closely related to the pathogen in antigen terms (divergent strains).
These also include
recombinant
(genetically engineered) vaccines containing vector strains of non-pathogenic bacteria/viruses (genes responsible for the synthesis of protective antigens of certain pathogens have been introduced into them using genetic engineering methods). Examples of genetically engineered vaccines include the hepatitis B vaccine, Engerix B, and the rubella measles vaccine, Recombivax NV.
Since live vaccines
contain strains of pathogenic microorganisms with sharply reduced virulence, then, in essence, they
reproduce in the human body a mild infection,
but not an infectious disease, during which the same defense mechanisms are formed and activated as during the development of post-infectious immunity.
In this regard, live vaccines, as a rule, create quite intense and long-lasting immunity.
On the other hand, for the same reason, the use of live vaccines against the background of immunodeficiency states (especially in children) can cause severe infectious complications.
For example, a disease defined by clinicians as BCGitis after administration of the BCG vaccine.
Live vakiins are used for the prevention of:
• tuberculosis;
• especially dangerous infections (plague, anthrax, tularemia, brucellosis);
• influenza, measles, rabies (anti-rabies);
• mumps, smallpox, polio (Seibin-Smorodintsev-Chumakov vaccine);
• yellow fever, rubella measles;
• Q fever.
An interval of at least 1 month is recommended between administrations of live vaccines, otherwise severe adverse reactions are possible and the immune response may be reduced.
3.
Killed vaccines
contain killed cultures of pathogens
(whole cell, whole virion).
They are prepared from microorganisms inactivated by heating (heated), ultraviolet rays, chemical substances (formalin - formol, phenol - carbolic, alcohol - alcohol, etc.) under conditions that exclude denaturation of antigens. The immunogenicity of killed vaccines is lower than that of live ones. Therefore, the immunity they evoke is short-lived and relatively less intense. Killed vakiins are used for the prevention of:
• whooping cough, leptospirosis,
• typhoid fever, paratyphoid A and B,
• cholera, tick-borne encephalitis,
• polio (Salk vaccine),
hepatitis A.
To killed vaccines
Also include
chemical vaccines
containing certain chemical components of pathogens that are immunogenic (subcellular, subvirion).
Since they contain only individual components of bacterial cells or virions that are directly immunogenic, chemical vaccines are less reactogenic and can be used even in preschool children. Anti-idiotypic drugs are also known
vaccines that are also classified as killed vaccines. These are antibodies to one or another idiotype of human antibodies (anti-antibodies). Their active center is similar to the determinant group of the antigen that caused the formation of the corresponding idiotype.
4.To combination vaccines
include
artificial vaccines.
They are preparations consisting of a microbial antigenic component
(usually isolated and purified or artificially synthesized antigen of the pathogen) and
synthetic polyions
(polyacrylic acid, etc.) - powerful stimulators of the immune response.
They differ from chemically killed vaccines in the content of these substances.
Antibody-mediated immunity—an example of RSV infection
Are antibodies necessary?
In children without antibodies (X-linked agammaglobulinemia), no severe course of RSV infections has been described. Also in a mouse model, animals lacking B cells exhibited virus clearance kinetics comparable to those of immunocompetent animals. As with most viruses, antibodies also play no role in primary RSV infection. Interestingly, upon secondary infection of B-cell-deprived animals, the virus was very quickly eliminated. This, however, is often associated with a more severe course of the disease. Antibodies are thus not necessarily required for protective immunity against RSV. It is clear that balanced B and T cell immunity is required to not only prevent viral spread but also to prevent clinical disease. However, a correlation between maternal levels of RSV neutralizing antibodies and severity of childhood illness following infection has not been found in all studies. Protection against RSV disease by antibodies becomes more evident with the prophylactic action of RSV-specific antibodies such as Respigam or Palivizu-mab. When taken regularly, Palivizumab (neutralizing IgG antibodies against RSV surface protein) was able to reduce the rate of RSV-related rehospitalizations in premature infants by 50%. Whether these results can be improved by optimizing the antibodies and their administration (dose and interval) is currently being intensively studied. The fact that even after natural RSV infection, despite high levels of neutralizing antibodies, RSV reinfection is possible, coupled with the limited effectiveness of maternal or transfused antibodies, rather argues against the idea that antibodies alone are sufficient.
Why do antibodies have limited effectiveness? As mentioned above, once the virus infects the target cell, the antibodies then remain ineffective. In addition, RSV, as a result of cell fusions, can spread from cell to cell, without the need for an extracellular phase. Whether IgA is probably more effective than IgG is not well known. In a mouse model, however, intratracheally administered RSV-specific IgA was less effective than IgG. There is no indication that patients with IgA deficiency suffer more frequently or more severely from RSV disease.
Can B cell immunity be induced in the presence of antibodies?
It is an important question for any vaccine that is given during the first months of life whether it, even in the presence of maternal antibodies (or in the case of RSV, even in the presence of prophylactically administered antibodies), can induce an adequate memory response. In this regard, there is good evidence from a mouse model that the presence of maternal antibodies prevents the live RSV vaccine from sufficiently activating infant B cells. During reinfection, there is no longer a sufficient level of neutralizing antibodies that can quickly resist viral replication.
How do T cells mediate antiviral immunity?
T cells are lymphocytes that, through highly specialized receptors, can recognize infected target cells. All nucleated cells have an enzymatic apparatus that can break down intracellularly synthesized proteins into peptide fragments. These fragments can bind to the MHC molecule and be transported to the cell surface.
Thus, the virus-infected cell presents viral fragments to T cells (Fig. 4). Contact of T-cell receptors with a complex of MHC and viral peptide leads, in combination with costimulatory signals, to activation of T-cells. What does clonal proliferation, differentiation and activation of antiviral effector mechanisms include? T cells mediate antiviral effector functions through the secretion of cytokines such as interferon-β and tumor necrotizing factor (TNF) or contact-dependent cytotoxicity (Fig. 5). These cytokines can either induce receptor-mediated intracellular antiviral effector mechanisms or activate other effector cells, such as macrophages. CD4+ T cells act primarily through cytokines, while CD8+ T cells generally exhibit cytotoxic function. An important molecular mechanism in this case is perforin-mediated induction of cell death; CD95-mediated apoptosis probably plays a lesser role in the control of viral infection. T cells cannot recognize free viruses in this way, but are capable of creating sterilizing immunity through the recognition and destruction of infected cells.
The study of antiviral T cells and their functions in humans, despite significant methodological progress achieved in recent years, is not yet satisfactory. Although, thanks to the use of MHC peptide tetramers or the ELISPOT method, it has become possible to count antiviral T cells. Particularly with regard to vaccine immunity, there are no well-measurable parameters that indicate whether a vaccine has sufficiently induced T-cell immunity to protect against clinical disease.
Vaccines. Definition, classification. History of the development of vaccination methods
Features of obtaining viral vaccines
4.Vaccines of plant origin
4. Anatoxins. Technology for producing toxoids (discussed in lecture No. 2)
Requirements for vaccines.
Introduction
Preventing the spread of infections through immunization is without a doubt one of mankind's greatest medical achievements. Vaccines currently prevent up to 3 million deaths annually. Over the 20th century, the average life expectancy of people has increased by about 30 years, which is largely due to mass vaccination.
Immunoprophylaxis is the use of immunological patterns to create artificial acquired immunity (active or passive).
For immunoprophylaxis use:
1. antigen drugs (vaccines, toxoids), when administered, artificial active immunity is formed in humans and animals;
2. antibody preparations (immune serums), with the help of which artificial passive immunity is created
Vaccines. Modern classification of vaccine preparations.
Vaccines are biological products that promote the creation of active immunity in the body of vaccinated people or animals..
Vaccines are obtained from pathogenic microorganisms themselves and their metabolic products (toxins).
Vaccines are administered for preventive (and less often for therapeutic) purposes.
E. Jenner received the first vaccine at the end of the 18th century. from the contents of smallpox capsules of calves (vacca - cow). Later, the vaccine was prepared on FE. Smallpox has been eradicated throughout the globe.
The doctrine of vaccines was developed by L. Pasteur. He proposed the attenuation of pathogens of infectious diseases under the influence of changes in external conditions.
Vaccines are classified according to the method of preparation:
1. Live vaccines are weakened or hereditarily modified pathogens. Prepared from avirulent strains of the pathogen. Essentially, they reproduce in the human body a mild infection, but not an infectious disease, during which the same defense mechanisms are formed and activated as during the development of infectious immunity.
They create intense and long-lasting immunity.
Not only live vaccines, but also killed vaccines, and even individual antigens have immunogenic properties.
2. Killed vaccines – obtained from pathogens killed in various ways. They are prepared from microorganisms inactivated by heating, UV rays, and chemicals under conditions that preclude denaturation of antigens. Killed vaccines are: heated, phenol, formaldehyde, alcohol, acetone, UV, ultrasound, etc.
Anatoxins - (toxins) are antigenic preparations obtained from microbial cell exotoxins, treated with formaldehyde and high temperature C0. In this case, the toxoid is devoid of the toxicity of the original exotoxin, but retains its antigenic properties. When toxoids are administered, antitoxic immunity is formed, since they induce the synthesis of antitoxic antibodies - antitoxins.
Chemical vaccines are various chemically extracted components of a microbial cell. Contains chemically pure pathogen antigens. They have weak immunogenicity.
5. Genetically engineered vaccines.
They are developed in virology, and hybrid vaccine strains are created. The genes responsible for its main antigenic markers are introduced into the genome of a known vaccine strain.
6. Combination vaccines . They are preparations consisting of a microbial antigenic component and synthetic polyions - powerful stimulators of the immune response.
Associated vaccines . They are a complex of killed vaccine and toxoid.
Here it is appropriate to recall the antigenic structure of a microbial cell.
T cell mediated immunity - an example of RSV infection
Is T-cell immunity necessary?
Children lacking T-cell immunity are extremely susceptible to advanced RSV infections. Patients with severe combined immunodeficiency (SCID) are unable to clear the virus. Also, in a mouse model, animals without T cells became chronic carriers of the virus. Selective depletion experiments show that CD4+ and CD8+ T cells can each partially compensate for each other, with CD8+ T cells clearly being more important. Despite the persistence of the virus, strikingly, only mild disease occurs—in patients with SCID, it is often the newly initiated T-cell reconstitution after bone marrow transplantation that results in severe clinical disease. T-cell-mediated elimination of the virus is accompanied by T-cell-induced immune pathology (Fig. 6). In general, T-cell immunity is thus required to control primary infection—antibody-mediated immunity is probably most often sufficient to control secondary infection.
Is T-cell immunity sufficient?
To answer this question, there is only data obtained from animal experiments. In a mouse model, B cell-deficient mice are completely protected from reinfection. In addition, transfusion of RSV-specific memory T cells into naïve animal recipients may interrupt RSV replication. RSV-specific T cells can, at least in animal models, also provide antiviral protection in the presence of B cells. Also in these experiments, the dual role of T cells in RSV infection became clear: immunopathologically mediated disease is the price of controlling the virus through the transfer of specific CD8+ T cells. In the mouse model, both processes are mediated by the same effector molecules interferon-—this also makes it difficult to control the pathogenic effects of T cells at the molecular level without impairing viral clearance.
Is it possible to induce T-cell immunity even in the presence of antibodies?
This is also why there is only a limited amount of data obtained from an experimental model. They indicate that, unlike B cell memory, RSV-specific T cell memory can be induced even when vaccination is carried out in the presence of transfused RSV-specific antibodies. Whether this T-cell immunity is sufficient to provide long-term protection against RSV disease is also unknown, nor is it known whether this knowledge can be transferred to humans.
In general, it is clear that T cells can make a significant contribution to antiviral immunity. An important goal remains to induce not only antibodies but solid memory T cells through vaccination. Since control of the virus can be carried out by T cells with the manifestation of immunopathology, it is very important to create a balanced B- and T-cell immunity (Table 1). Unfortunately, there are currently no reliable measurement methods that would allow the quantification of protective virus-specific T-cell responses. Antibodies should therefore continue to primarily serve as surrogate markers for the induction of antiviral immunity by vaccination.
RSV-lot100 - immunological explanations
Based on these results, the misdirected immunity caused by RSV-lot100 became clearer. Children vaccinated with this vaccine even developed high titers of antibodies against the RSV-F protein. These antibodies, determined by ELISA, however, showed only minor activity in the neutralization test. It is likely that formaldehyde inactivation particularly altered the epitopes of DSV surface proteins against which protective neutralizing antibodies should have been induced. It may also have been significant that the vaccine did not induce any local mucosal-associated immunity. Since the killed vaccine, due to the lack of replication, also could not cause any good response of CD8+ T cells, the virus was not eliminated quickly enough and could further spread in the lower respiratory tract of these children. In addition, the vaccine likely induced a Th2 immune response, which, upon contact with RSV, led to reactivation of CD4+ T cells with increased local production of IL-4, IL-5 and IL-10. These cytokines caused an influx of eosinophilic granulocytes with the secretion of their mediators, resulting in inflammation and bronchoconstriction. Finally, the formation and deposition of immune complexes over complement activation contributed to pulmonary pathology. A similar immune complex reaction was also observed in children with an atypical course of measles after vaccination with a previously used formalin-inactivated measles vaccine. This point is illustrated by the fact that not only T cells, but also antibodies can cause pathological immune responses (Table 2).
Attenuated live vaccine as an ideal vaccine?
The goal of inducing balanced immunity against RSV or other viruses is likely to be achieved by local vaccination with an attenuated live vaccine. The advantages are the physiological route of immunization with the activation of local and systemic immunity, as well as the optimal balance between B-cell and T-cell immunity.
The difficulty in creating such a vaccine lies in the difficulty of selecting the correct degree of attenuation. If you attenuate too much, no sufficient protection will be achieved. If the attenuation is too weak, you should expect side effects typical of an infection, such as, for example, with RSV, blockage of the airways with refusal to drink or sleep disturbances. Also, rare incidents such as the incidence of sudden infant death should be carefully analyzed in vaccine studies, as has been shown by the increased incidence of intussusception following vaccination with locally administered live rotavirus vaccine. In the current development of a vaccine against RSV, the issue of correct attenuation continues to remain the main problem, even if in the meantime it has become possible to manipulate the RSV genome and quite purposefully induce attenuation mutations. A number of promising candidate vaccines still require a long period of experimental work before their use in adults, children, and finally before testing on seronegative infants (Fig. 7). So far, however, none of the viral isolates show the correct size attenuation. Even if attenuated live vaccines seem to be an ideal vaccination strategy from an immunological point of view, numerous problems still need to be solved in practice.