Indications for vaccination "Vaxigrip"
Vaccination is recommended for all individuals and, above all, for those who are at increased risk of contracting influenza, especially if influenza is added to existing diseases:
- Young children (under 1 year old)
- Children attending kindergarten, school, sports and children's sections, clubs.
- Adults over 65 years of age.
- People with chronic respiratory diseases, including bronchial asthma, renal failure, hemoglobinopathies and immunodeficiency conditions.
- Patients with cardiovascular diseases.
- Patients with chronic renal failure.
- Patients with chronic metabolic disorders, including diabetes mellitus.
- Children and adults with immunodeficiency conditions, patients receiving immunosuppressants, cytostatics, radiation therapy or high doses of corticosteroids.
- Children and adolescents from 6 months. under 18 years of age who have been receiving medications containing acetylsalicylic acid for a long time and are therefore at increased risk of developing Reye's syndrome due to influenza infection.
- Medical personnel, teachers, doctors, public transport drivers: all those who come into contact with large numbers of people every day, as well as members of their families.
Flu vaccination
Most people interact with each other in teams. Children attend kindergarten, school, colleges and universities, and adults go to work. During the period of rising incidence of influenza, one of the important criteria for preparedness for this phenomenon is the size of the immune layer. Immune layer - the number of people in a team (%) vaccinated against influenza. Any person (adult or child) vaccinated against influenza is a barrier to the spread of the virus. If an infected person ends up in a group, then the more vaccinated people in this group, the less likely the disease will spread like an avalanche. Consequently, the higher the percentage of vaccinated people in a team, the fewer ways of transmitting the virus. As studies show, in a team where the immune layer tends to 100%, the incidence of influenza is reduced by 12 times, 50% - by 4.5 times.
It is necessary to take into account the timing of the formation of immunity after vaccination. It is very important to get vaccinated in advance so that when the disease rises, you and your children are fully protected. The period October-November is traditionally characterized by an increase in the frequency of acute respiratory infections. People begin to get respiratory infections, and women often have to take sick leave to care for their children. Manifestations of rhinitis or a rise in temperature above 37 degrees are regarded by doctors as a contraindication to vaccination. It is very difficult to get vaccinated during this period. Therefore, in order to create the maximum immune layer in the team (at school, kindergarten, at work), it is recommended to get vaccinated at an earlier date, namely in September.
Vaccination in September provides the following benefits, which are related to each other:
- Virtually no colds
- Mothers do not take sick leave to care for their children
- There are no contraindications to vaccination (rhinitis, slight rise in temperature)
- Immunity is formed 14 days after vaccination, and by October the vaccinated person (adult or child) has developed antiviral protection
Vaccination is an opportunity to avoid influenza and the serious complications that accompany infection. Vaccination also helps reduce financial losses, expressed in reduced income during the period of loss of ability to work and reduced costs associated with treatment. And the most important point: if you are vaccinated, you will not bring the flu virus into your home and will not cause illness to your loved ones. Early vaccination allows you to create all the conditions for maximum protection of the team during the period of increased incidence of influenza.
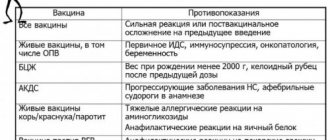
Contraindications
Only a doctor can decide whether Vaxigrip is suitable for vaccination
Vaxigrip is contraindicated if you have a history of an allergic reaction to any component of the vaccine.
Vaxigrip vaccination is contraindicated in the following cases:
- If a child or adult is allergic (hypersensitivity) to the active substances of the vaccine or any of the ingredients - egg whites or chicken whites, neomycin, formaldehyde or octoxynol-9.
- If the child has an illness with high or moderate fever or acute infection.
Possible side effects
The following adverse reactions may be observed during vaccination: headache, sweating, myalgia, arthralgia, fever, malaise, chills, fatigue, dizziness, insomnia, vomiting, fever. Local reactions may include: redness, swelling, pain, induration, ecchymosis. Reactions usually resolve within 1-2 days and do not require treatment.
Come get vaccinated at MiracleChildren. A full range of vaccines for children and adults, family vaccinations - at a special price!
EpiVacCorona protects against coronavirus. Or not
A long-awaited event: the results of phase 1-2 clinical trials of the EpiVacCorona vaccine against COVID-19, developed by the State Research Center for ViB “Vector” of Rospotrebnadzor, were published by the journal “Infection and Immunity”. The journal is much less prestigious than The Lancet, in which the developers of Gum-COVID-Vac published. The two-year impact factor according to the RSCI for “Infections and Immunity” is 0.775.
One way or another, now there is more detailed information about the vaccine: a detailed description of the selection of participants, inclusion criteria, vaccination procedure, side effects (very minor). And the main thing is the features of the humoral response, that is, the production of antibodies.
What is the vaccine made of?
Until now, the sources of information were interviews with Vector employees and in the media, descriptions of inventions for patents (, ,), as well as answers from developers to questions from CI participants: in and. From the patents we were able to find out exactly which sections of the amino acid sequence of the S-protein were selected for testing on animals and then for the “human” vaccine: there seems to be no secret in this, but this was not announced anywhere.
The description for patent No. names regions S454-477, S1179-1200, S1189-1209, that is, one peptide from the receptor-binding domain of the RBD subunit S1 and two overlapping ones from the S2 subunit. The numbers are the numbers of amino acids in the S protein of the coronavirus, the same one that, in the form of a trimer, forms the “spikes” of the virus and binds to the cellular receptor ACE2.
Specialists not involved in the development wondered how these peptides were chosen and why they were chosen.
.
There is no detailed answer to this in the publication. It said that " in silico
of peptide fragments representing known viral antigens" was used and the most effective combinations were selected in animal experiments. It also said that data on the well-studied S protein of SARS-CoV-1 were taken into account; Let us remember that the development of the vaccine began a year ago, when much less was known about the new coronavirus than it is now. Epitopes associated with possible antibody-dependent enhancement of infection, as well as epitopes similar to regions of human proteins, were excluded. (Antibody-dependent enhancement of infection is a rare phenomenon when an antibody, binding to the virus, promotes not its destruction, but its penetration into immune cells. Signs of ADUI were observed in experimental conditions for other coronaviruses, and many feared that it was possible for SARS-CoV- 2.) We also gave preference to the most conserved regions of the protein, which are least likely to be affected by mutations.
Binding of an antibody to the receptor-binding domain can, of course, prevent the virus from interacting with the cell (although not all epitopes in the receptor-binding domain of the RBD are neutralizing). The role of epitopes from S2 (the “leg” of the S protein) is not entirely clear; perhaps the binding of antibodies to these regions prevents the fusion of the virus and cell membranes. But there is another difficulty with peptides S1179-1200, S1189-1209: they contain a glycosylation site, that is, an amino acid to which a carbohydrate chain is attached in the virus protein. Naturally, the synthetic peptide in the vaccine does not contain it, hence the question: will antibodies to a peptide with a glycosylation site, but without carbohydrate, correctly recognize the viral protein.
To be immunogenic, the molecule must be large enough, so a short peptide is covalently attached to a carrier protein. This construct is sorbed onto an adjuvant (aluminum hydroxide). In animal experiments, the role of the carrier protein was played by molluscan limpet hemocyanin (KLH), a powerful activator of T helper cells, well known for its immunostimulating properties. It was part of the EpiVacEbola vaccine. However, the EpiVacCorona vaccine used a different carrier protein
is a chimeric protein produced in Escherichia coli that includes the complete sequence of the nucleocapsid (N-protein) of SARS-CoV-2.
Alexander Ryzhikov, head of the Department of Zoonotic Infections and Influenza of the State Scientific Center for Virology and Biotechnology “Vector”, said at a meeting with the initiative group of trial participants that this choice was due to the high cost of hemocyanin, and in addition, the N-protein is “an invaluable source of a large number of T-helper epitopes of coronavirus " At the same time, it is possible that the replacement of the carrier led to lower antibody titers in humans compared to those titers that were obtained in animal experiments (very high indeed).
“I don’t see a soft way out of this situation”
There is no quantitative data yet on the protective effectiveness, that is, the effect of the vaccine on the likelihood of contracting COVID-19. Phase 1-2 of the CT began in July 2021 and will end on May 18, 2021, then, obviously, there will be final data on the proportion of cases among those vaccinated and among those who received a placebo. The article reports one vaccine recipient who became ill with COVID-19 and one in the placebo group. However, 100 people, of whom 43 received a placebo and the rest received a vaccine, is in any case not enough for reliable statistics. An interim response on post-registration tests, in which 3,000 people are taking part, will be prepared no later than mid-April, said Vladimir Petrov, head of the information and analytical department of the State Research Center for ViB “Vector”.
The immune response to the EpiVacCorona vaccine, that is, the appearance of antibodies and cellular responses in vaccinated people, has been discussed since the beginning of the year. In January, the press service of Rospotrebnadzor stated that “according to the results of phases 1-2 of clinical trials, the immunological effectiveness of the EpiVacCorona vaccine is 100%.” It was emphasized that the immune response must be detected using a special test in which antibodies interact not with the full-length S-protein of the coronavirus, as in most commercial tests, but with peptides similar to those included in the vaccine. This raised a new question: if so, will the antibodies generated after vaccination with EpiVacCorona interact with the S protein of the real virus?
CI participants, frustrated by the lack of information, began conducting their own research. Earlier this week, they published an open letter stating that among those vaccinated there were sick people, including those hospitalized, and that “120 participants in phase III clinical trials and 19 vaccinated as part of civil vaccination were tested for antibodies using a test system recommended by Rospotrebnadzor . No antibodies were detected in 30% (adjusted for placebo for clinical trial participants).”
Moreover: protective effectiveness is largely determined by neutralizing antibodies. In experiments organized by the initiative group, it was not possible to detect neutralizing activity in any of the dozens of serum samples from vaccinated people. The neutralization reaction was carried out in several laboratories. The website epivakorona.com describes in detail the results obtained by Dr. Alexander Chepurnov, leading researcher at the Federal Research Center for Fundamental and Translational Medicine SB RAS, formerly head of the Vector Laboratory of Particularly Dangerous Infections. Alexander Chepurnov has experience working with SARS-CoV-2 and often gives comments to the media. He is also the author of the popular science book “Virologist: The Cost of Mistake” about the Marburg virus.
And then the most interesting part. These results directly contradict the data presented in the article. In the first phase, we recall, 14 people participated, in the second - 86, but half received a placebo. Of the 57 vaccinated people, all of them developed antibodies. And not only to the vaccine antigens, but also to the full-length SARS-CoV-2 virus, inactivated by beta-propiolactone. Neutralizing activity was also observed in all vaccinated individuals, with titers ranging from 1:20 to 1:160. The developer's publication describes in detail the method for determining neutralizing antibody titers: the text includes small details that are usually placed in applications, down to the number of washes of wells with cells.
How could this happen? It is well known that absolute values of neutralizing titers obtained in different laboratories are difficult to compare. The conditions for the neutralization reaction, methods for detecting cell damage, and the criteria for the “neutralizing titer” themselves differ: for example, the maximum dilution of human blood serum at which the virus cannot infect cells in culture can be called neutralizing, or a dilution at which the number of infected cells is halved. But the difference between “everyone has antibodies” and “no one has” is too great for methodological nuances.
Andrey Krinitsky answers the question
, CEO of the company and founder of the epivakorona.com project.
“There are cases in which a specific technology does not play a role. In this situation, either someone made a mistake (multiple) during the experiment, or he is lying.
Alexander Chepurnov could not have made a mistake, since the experiment contains “controls” (samples from those vaccinated with Sputnik V or those who have recovered from the disease, and the researchers did not know which samples belonged to whom. - PCR.NEWS
). The experiment was repeated many times in the same laboratory. And exactly the same data were obtained in two other independent laboratories. Taking into account the great resonance and public importance, just in case, we will repeat Chepurnov’s experiment again, this time in Moscow. This will be the fifth such inspection and the second on our initiative.
I don’t see a beautiful and soft way out of this situation - the two sides have diametrically opposite results of the experiment. This means that at least one of the two sides is doing very badly. Until we find a laboratory that dares to openly and officially publish the results of such an experiment, I can only ask influential people, just like us, to privately order a repeat of the experiment and act on its results. You don’t need to take Vector’s word for it, you don’t need to trust us - repeat and see for yourself. It’s a matter of life and death for many people, it’s really worth it.”
The final part of the vaccine developers' article states that "high titers of virus-specific antibodies are not necessarily associated with protection against COVID-19." The authors note that the N-protein in the vaccine, although it is not a target for neutralizing antibodies, unlike the S-protein, can contribute to the emergence of virus-specific T- and B-memory cells, and memory T-cells can persist longer. -cells. It must be understood, however, that a peptide vaccine, unlike a vaccine based on adenovirus or mRNA, cannot promote the production of cytotoxic T cells (killer T cells, CD8+ T lymphocytes), that is, we are talking only about T helper cells (CD4+) , and above all about those that activate B-lymphocytes that produce antibodies.
Unfortunately, the article does not say anything about the study of T-cell response.
About epitopes and antibodies
We asked Kirill Skripkin
. Kirill is a biophysicist, he closely monitors information related to EpiVacCorona, and his comments on social networks are always informative.
Kirill, the first question is about the peptides that were used in the vaccine.
Among my friends, you were the first to find a patent where these sections were named: S 454-477, S 1179-1200, S 1189-1209. That is, one peptide from the receptor-binding domain of the RBD subunit S1 and two overlapping ones from the S2 subunit. These peptides include epitopes described elsewhere, regions to which neutralizing antibodies, such as or , .
Does this mean that the formation of neutralizing antibodies to the vaccine is possible? Critics of this vaccine have a reasonable objection that the epitopes described in the articles linked above are not linear epitopes, but conformational ones. Therefore, a linear amino acid sequence from this epitope in a vaccine peptide cannot generate neutralizing antibodies. But the authors of the first work claim that they mapped exactly linear epitopes. In addition, according to the same authors, antibodies to conformational epitopes may retain some affinity for the linear peptides that make up the epitope.
The other two peptides: as far as can be understood from statements to the general public about the “three lines of defense”, antibodies to them should prevent the fusion of the virus with the cell, since the
S 2 subunit is responsible for fusion.
Is it effective? Have other vaccine developers done this? In your opinion, why were the overlapping peptides chosen? To answer the first question, you need to understand what is meant by the word “effective”? Efficacy, effectiveness or efficiency? (That is, the reduction in disease incidence in a vaccinated group of people compared to an unvaccinated group under “ideal” controlled conditions, such as clinical trials; the same in real-world settings; or cost-benefit ratio. - PCR.NEWS
.) If efficacy, then based on the intermediate results of phase 1-2 CT we can say that so far yes, but we need to wait for the results of the third phase. The effectiveness can only be learned from the results of civil vaccination if they are revealed by Rospotrebnadzor, and the efficiency should be assessed by the planning and economic department of the Ministry of Health.
On the second question: the developers of the peptide vaccine COVAXX - UB-612 from Taiwan also use peptides from the S2 subunit and N-protein in their vaccine.
On the third question: I always believe in the best, so I think that using two overlapping peptides with a glycosylation site in them is some kind of cunning plan. Although the new patent from Vector contains only one peptide from the S2 subunit: S1179-1209.
The authors write that they chose peptides rather than full-length
S protein because they were concerned about an antibody-dependent increase in infection. N was chosen as the carrier . But the use of full-length N protein as a carrier of peptides cannot lead to ADUI? And by the way, has ADID in SARS - CoV -2 infection been registered at all?
Thanks to the respected Olga Matveeva, we know that the N-protein of the first SARS caused a vaccine-associated increase in infection in mice (articles and years). There is currently no reliable information on the registration of ADUI during SARS-CoV-2 infection.
Immunogenicity was determined in three ways: antibodies to peptides in the vaccine, antibodies to the inactivated
SARS - CoV -2 virus, and antibodies neutralizing viable SARS - CoV -2.
Do these experiments answer the question of whether antibodies generated by a vaccine will interact with the actual virus? Yes, in a neutralization experiment, the ability of vaccine antibodies to prevent the penetration of a viable SARS-CoV-2 virus into Vero E6 cells, which carry ACE2 molecules on their surface, was shown.
It is difficult to compare different experiments to establish neutralizing activity, but let's try.
In phase 3 of the Gam-Covid-Vac clinical trial, 100 people had a geometric mean titer of neutralizing antibodies on day 42 , all but three had antibodies.
In the EpiVacCorona publication, the titers of neutralizing antibodies after two vaccinations range from 20 to 160, the geometric mean titer is 68 on the 35th day, seroconversion is 100%. The methods and definition of “neutralization titer” differ in these works. But at least roughly, who has more credits? No, it is completely wrong to compare the results of two completely different neutralization methods. Only the results of comparison of neutralizing antibody titers in vaccinated and convalescents for both types of neutralization reactions can be correlated with each other. In Gamaleya such a comparison was made, but for some reason in “Vector” it was not.
At the same time, the authors emphasize that protection against
COVID -19 is possible even at low titers. They also note that in experiments on primates, neutralizing antibodies appeared but disappeared four weeks before the experiment in which monkeys were infected with the virus, but protective effectiveness was demonstrated. It is said that the N protein was chosen because it contains epitopes of cellular immunity.
But at the same time, the article does not contain data on the cellular immune response of CT participants. What can be said about the cellular immunity induced by a peptide vaccine? As soon as the plasma cells that produce neutralizing antibodies disappear, these antibodies themselves disappear. The average half-life of immunoglobulin G is 21 days. That is, neutralizing antibodies in primates were again produced by immunological memory cells. This could be confirmed if the titer of neutralizing antibodies was determined in primates after a stress test, but the authors of the article are silent about this. There is a statement about cellular immunity by the respected Alexander Ryzhikov: “As for the cellular immune response, it is present and shifted, as we observed in primates and also in humans, into the so-called Th2 type of immune response, that is, humoral immunity dominates. And CD8 cells (cytotoxic lymphocytes) are weakly induced by this type of vaccine.”
PCR.news is monitoring developments. Obviously we'll have more information soon.
Source
A.B. Ryzhikov et al. // Single-blind, placebo-controlled, randomized study of the safety, reactogenicity and immunogenicity of the EpiVacCorona vaccine for the prevention of COVID-19 in volunteers aged 18–60 years (phase I–II). // Infection and immunity. 2021, 11, 2; DOI: