Intramuscular administration of drugs
Medicines prescribed by a doctor are introduced into the patient’s body enterally (through the digestive tract) and parenterally (bypassing the gastrointestinal tract).
One of the most popular methods of parenteral drug administration is intramuscular injection, a procedure that every nurse should be familiar with. Intramuscular injections are carried out in the treatment room of a hospital or outpatient medical facility, in the ward directly in the patient’s bed and at home as prescribed by the local doctor.
A certified or accredited specialist who has a state diploma of completion of a secondary or higher medical educational institution in the specialty: “Nursing”, “Midwifery”, “General Medicine”, “Pediatrics” has the right to administer intramuscular injections in medical institutions and at home.
The purpose of the procedure is to introduce a medicinal solution into muscle tissue.
Indications for intramuscular injections are determined exclusively by the attending physician or the doctor on duty.
Contraindications . Determined by a doctor. There should be no inflammatory and/or degenerative processes at the injection site (ulcers, rashes, burns, etc.)
Advantages of the method . Exact dosage. Rapid entry of the drug into the body, although not lightning fast (as with intravenous administration). Quite accurate dosage of the drug.
Indications and puncture sites
Intravenous jet administration of medicinal substances is carried out once or as a course of treatment:
- when providing emergency care
- if it is necessary to quickly introduce the drug into the bloodstream
Indications for intravenous injections are determined solely by the doctor. A nurse performs a procedure as prescribed by a doctor.
To administer the drug into the venous lumen, venipuncture (from the Latin vena -
vein,
punctio -
to prick). It is easier to puncture well-defined veins. Places where veins are close to the skin:
- elbow bends
- back of the hand
- forearm
- temporal veins - in newborns
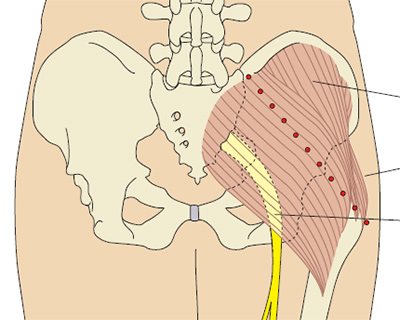
Possible sites for administering drugs into the muscle
Intramuscular injection is performed in one of the anatomical areas:
- superior outer quadrant of the buttock (gluteus maximus)
- thigh, medial anterolateral surface (rectus femoris and lateral head of quadriceps femoris)
Read also: Hand treatment for medical personnel: levels, washing technique

- shoulder (deltoid muscle)
The necessary conditions
Intravenous injection is performed in a manipulation room, in a hospital ward or intensive care unit. In exceptional cases, namely in life-threatening situations, intravenous injection can be performed at home or in transport. The drug, its dosage, frequency and duration of administration are chosen only by the doctor. Despite the presence of other routes of administration, intravenous injections (techniques, algorithms) are a mandatory skill for any healthcare worker.

Everything that comes into contact with the vein must be sterile, since the medicine goes directly into the general bloodstream. Before performing the injection, you need to clarify all the details on the prescription sheet, and if anything is unclear, ask your doctor. It is also necessary to talk with the patient and find out from him whether he has previously had an allergic reaction to the drug, and how he felt after the injection. Particularly nervous patients should be reassured by explaining in simple words the purpose of administering the drug. Immediately before the injection, you need to wash your hands with soap and treat them with an antiseptic.
Preparation for the procedure
In accordance with modern requirements, before administering an intramuscular injection, the nurse must:
- Invite the patient into the treatment room or approach him in the ward, introduce yourself, identify the patient and inform him about the purpose and progress of the upcoming procedure, emphasize that everything is done as prescribed by the attending physician
- Make sure that the patient has informed consent for intramuscular administration of the drug with a note about the tolerability of the administered drug. If documentation is missing, check with your doctor for further steps.
- Wash hands hygienically and dry with a disposable paper towel. Treat the skin of your hands with a special antiseptic, do not dry them, wait for them to dry. Wear a mask and non-sterile gloves.
- Take a bottle or ampoule with the medicine, check the expiration date, check the name with the doctor’s prescription, make sure there is no external damage, and evaluate the transparency of the solution.
- Take a syringe of the required volume with a needle of sufficient length and thickness, check the expiration date and integrity of the packaging, and open the syringe.
- Draw up the medicine into the syringe.
- When taking a drug from an ampoule : check the name, appearance, dosage and expiration date of the drug, shake the ampoule so that the solution is in its widest part, file the neck, wipe the neck with an antiseptic napkin, break the neck, draw the drug.
- When taking a medicine from a bottle : check the name, appearance, dosage and expiration date of the medicine, use scissors or tweezers to bend the part of the cap covering the rubber stopper, wipe the stopper with an antiseptic napkin, place the needle through the stopper into the bottle at an angle of 90 degrees so that the cut was inside the bottle, turn the bottle upside down, draw the solution into a syringe.
- Replace the syringe needle with a sterile one, release the air from the syringe without removing the cap from the needle, and place the syringe in a sterile tray. Place wipes for treating the injection field in the same tray.
- Invite the patient to take a comfortable position lying on the couch.
- Select the injection site, inspect and palpate it for signs of inflammation and infiltration. If any, change the injection site and inform your doctor.
Read also: Intravenous infusion: execution algorithm, indications, complications
Basic Information About IV Injection

In the treatment process, practical medicine cannot do without drugs that enter the body in several ways. Intravenous injection provides extremely valuable assistance in cases where an emergency condition has arisen.
In this case, drugs are delivered into the blood immediately with prescription dosage accuracy, and the desired concentration in the blood will remain for a long time thanks to repeated injections.
The introduction of medicinal drugs into a vein will be beneficial when the medicine cannot be swallowed or the standards for the implementation of the drug provided for its ingestion through the blood.
How to give intravenous injections?
Intravenous injection is prescribed in areas saturated with swollen veins: on the forearm, in the antecubital fossa and on the hand. The injection algorithm includes the following steps:
- detection of a filled vein,
- insertion of a needle by puncture into a vein,
- bending the person's arm at the elbow joint to stop bleeding from the puncture site.
The extended injection algorithm is performed in eleven steps:
- Prepare the patient for the injection - sit him on a chair or couch.
- Before injecting into the vein, place the elbow bend of your arm on a thick cushion.
- Draw the medicine into the syringe.
- Attach a venous tourniquet above the elbow to obtain blood flow to the veins.
- Ask the patient to use his fist while feeling the blood-filled vein.
- Medicines will be injected into the intended location.
- Disinfect the injection site twice with alcohol.
- The needle is inserted (cut upward), the tourniquet is untied, and the fist is unclenched.
- The drug is administered slowly, a couple of tenths of a ml remains in the syringe.
- The needle is removed from the vein, a cotton swab is applied to the injection site, and the arm is bent.
- It is recommended to keep your hand in a bent position for five minutes (no bruising will form).
Important! It is possible to protect the patient from infection in the blood by observing sanitary hygiene: disposable gloves for the nurse, sterility of the needle and the injected drug is ensured by the factory packaging conditions. At the end of the procedure, the injection site is covered with a cotton swab with alcohol.
Blood sampling from a vein and any administration of medications into a vein are carried out by trained medical personnel.
Technique for intravenous injection
The duration of administration of medications into a vein lasts ten minutes. The injection technique allows an experienced nurse to inject into a vein painlessly and so quickly that you don’t have time to get scared. Typically, the drug is injected into a vein in the elbow area.
If it is not possible to find blood-filled veins in this area, then other veins located on the back of the hand are taken for injection. The medicine is not injected into the veins in the legs for the reason that the risk of blood clot formation increases.
The algorithm for correctly performing an injection contains the following procedure:
- The syringe is taken with the right hand, the needle cannula is held with the index finger.
- The syringe barrel is compressed with the other fingers of the hand.
- The vein is palpated again, the future injection site is treated with a new swab, and the left hand fixes the skin.
- The patient clenches his fist.
- The hand holds the syringe almost parallel (at an angle of 15 degrees) to the injection site, the needle is cut upward.
- A puncture is made, the needle passes one third between the skin and the vein, then the wall of the vein is pierced, this action is controlled by the feeling of “failure”.
- Pull the plunger of the syringe slightly, blood will appear in the cylinder, which proves the presence of a needle in the vein.
- The tourniquet is removed, the fist relaxes
- Re-check the needle in the vein.
- Slow injection of the drug; part of the drug remains in the cylinder and is not administered.
- The syringe is removed, a cotton swab with alcohol is applied, and the arm is bent.
- Hold your hand in a bent position for 5 minutes, there will be no bruising.
Intramuscular injection: algorithm of actions when performing the procedure
- Select the injection site.
- Treat the patient's skin with antiseptic wipes twice. First treatment - an area of about 10*10 cm is wiped with a napkin in the same direction. Then the second treatment - with a second napkin, the same area is 5 * 5 cm.
- Stretch the patient’s skin in the area of the intended puncture with the thumb and index finger of one hand to increase the volume of the muscle and facilitate insertion of the needle.
- Take the syringe in the other hand (index finger on the piston, little finger holding the needle cannula, the rest on the cylinder), place it perpendicular to the surface of the patient’s body. For intramuscular injections into the thigh and shoulder, the syringe must be held at an angle, like a pen, to prevent damage to the periosteum.
- With a quick, easy movement, insert the syringe needle at an angle of 90 degrees to 2/3 of its length. Pull back the plunger slightly to make sure there is no blood in the syringe.
- Holding the cannula of the needle and pressing the piston, slowly inject the medicinal solution into the muscle.
- Pressing the antiseptic napkin to the puncture site, quickly remove the needle.
- Continuing to press the napkin, lightly massage the injection site.
- Place the napkin and syringe in the waste tray.
- If necessary, apply a sterile adhesive bandage to the puncture site.

Determining the area for subcutaneous injection
In order not to harm yourself, you need to learn how to correctly determine the injection sites and alternate zones [4]:
- arms - the outer surface of the shoulder in the area under the deltoid muscle and not reaching the elbow joint;
- hips - the front surface 10-15 cm from the groin and 10-15 cm from the knee along the center line of the leg; posterolateral surface from the buttock and not reaching the popliteal fossa;
- buttocks: outer upper quadrant (draw two imaginary lines: horizontal - from the place where the intergluteal gap begins to the greater trochanter of the femur and a vertical line perpendicular to it) or slightly higher, as far as subcutaneous fatty tissue allows;
- belly - approximately 5 cm from the navel, outside the linea alba.
Subcutaneous injections should be administered where the subcutaneous fat layer is most developed so that the drug does not inadvertently enter the muscle [4]. Within each zone there is space for multiple injections. As you gain the skill of administering injections yourself, you will be able to distribute zones more and more compactly.
End of the procedure
- Place used needles in a Class B sharps waste container using a needle remover.
- Place syringes, gloves, used wipes in a Class B waste container.
- Wash your hands hygienically and dry with a disposable towel.
- 10-15 minutes after the procedure, inquire about the patient’s well-being and his reaction to the administration of the drug. If there are complaints about the patient’s health, inform the attending physician.
- Enter information about the intramuscular injection procedure into the medical documentation.
What injections are given to pregnant women to thin the blood?
The choice of blood thinner should be approached with caution. Not all of them are safe for the fetus and can lead to serious consequences.
Several groups of drugs are registered as anticoagulants:
- Coumarin derivatives;
- Heparin and its analogues;
- Indirect factor Xa inhibitors;
- Direct thrombin inhibitors.
During treatment, drugs can act in two ways:
- Pass through the placenta and have a negative effect on the baby.
- Cause bleeding.
Heparin and its analogues are considered the only safe drugs. It does not pass through the placental barrier and is not capable of causing bleeding in a pregnant woman.
The most commonly used low molecular weight heparins are Fraxiparine and Clexane. In the instructions for them, pregnancy and breastfeeding are indicated as contraindications. But if there is a high risk of blood clots in the mother, the drug is used to prevent severe complications. The medicine is administered subcutaneously by injecting into the fatty tissue of the abdomen.
Are blood thinner injections safe for mother and fetus?
It has been reliably confirmed that injections of the coumarin derivative Warfarin pose a danger to the fetus. It crosses the placenta and can cause bleeding in the fetus. The teratogenic effect consists of disruption of the formation of bones and cartilage, softening of the epiphyses of the extremities, nasal hypoplasia, and pathology of the central nervous system.
Low molecular weight heparins Fraxiparin and Clexane do not pass through the placental barrier, and therefore are not capable of having a teratogenic effect. Statistical studies confirm the safety of these drugs for the fetus.
All women undergoing anticoagulant treatment during pregnancy should have their platelet levels monitored. First, before starting the drug, the initial cell level is determined. Then, every three weeks, the platelet count is monitored using a blood test. Their decrease is an unfavorable symptom.
Heparins are discontinued 12-24 hours before the expected delivery (caesarean section or amniotomy and labor induction).
Injections or blood thinners: which is better?
The choice of a specific form of the drug should be made by the doctor based on the indications. It is impossible to say which drug is better, tablets or injections. Because each situation requires an individual approach.
Women with recurrent miscarriage, a history of severe pereclampsia or HELLP syndrome, and a hereditary risk of early stroke are at risk of developing thromboembolic complications. They can do without heparin injections. But small doses of aspirin are prescribed as an anticoagulant - 75-162 mg/day. The use of low molecular weight heparin in the form of injections is necessary in severe situations where there is a high risk of blood clots.
Yulia Shevchenko, obstetrician-gynecologist, especially for Mirmam.pro
Intramuscular injection: possible complications
- Needle breakage
- Traumatization of the periosteum
- Damage to nerve trunks
- Formation of infiltrates, hematomas, abscesses
- Oil, suspension embolism
- Thrombophlebitis
- Soft tissue necrosis
- Allergic reactions
- Infection with parenteral hepatitis, HIV infection
Read also: Measuring body temperature: algorithm. Types of thermometers
All facts of unusual reactions and complications after them must be documented. If you suspect a complication has developed, you must inform your doctor and senior nurse. Early detection of changes in the patient’s well-being will make it possible to alleviate or prevent the development of a full-fledged complication that may result from an intramuscular injection.
Types of Veins
Type 1:
a well-contoured vein (the vein is clearly visible, clearly protrudes above the skin, is voluminous, the lateral and anterior walls are clearly visible); upon palpation, almost the entire circumference of the vein can be felt, with the exception of the inner wall.
2-type:
weakly contoured vein. Only the anterior wall of the vessel is very clearly visible and palpated; the vein does not protrude above the skin
3rd type:
uncontoured vein. The vein is not visible, it can be palpated deep in the subcutaneous tissue (this can only be done by an experienced nurse), or the vein is not visible or palpated at all.
The next indicator by which veins can be divided is fixation in the subcutaneous tissue (how freely the vein moves along the plane). Before making the injection, you need to apply a tourniquet to expose and fix the vein.
Where to put syringes and balls after injection?
The intramuscular injection algorithm assumes that everything that comes into contact with the blood is biological waste. Therefore, the manipulation room should have the following containers:
- for washing syringes;
- for soaking used syringes;
- for used needles;
- for used cotton balls.
The containers are filled with a disinfectant solution, which is changed daily. The syringe with the needle is washed in the solution, then the needle and cap are disconnected and placed in a separate container. The washed syringe is disassembled and placed in another container. The balls are soaked separately. Syringes, needles and balls washed in a disinfectant solution are disposed of under an agreement with a disinfection institution.
How is an intravenous injection given?
The vein injection algorithm consists of the following steps:
- The doctor discovers a filled vein
- Inserts the needle at an angle, thereby puncturing the vein
- Injects the medicinal substance into the venous bed.
- Removes the syringe with the game and bends the arm at the elbow joint to stop bleeding from the puncture site
It is important to remember that puncture of a vein is a rather dangerous procedure and can lead not only to damage to the walls of the vein or puncture through it, but also to infection directly into the patient’s blood. Therefore, do not perform intravenous injections yourself, contact professional medical personnel
It is also worth paying careful attention to sanitary hygiene standards: disposable gloves, disposable syringes and needles, disinfection of the area around the vein puncture site
The necessary conditions
Intravenous injection is performed in a manipulation room, in a hospital ward or intensive care unit. In exceptional cases, namely in life-threatening situations, intravenous injection can be performed at home or in transport. The drug, its dosage, frequency and duration of administration are chosen only by the doctor. Despite the presence of other routes of administration, intravenous injections (techniques, algorithms) are a mandatory skill for any healthcare worker.

Everything that comes into contact with the vein must be sterile, since the medicine goes directly into the general bloodstream. Before performing the injection, you need to clarify all the details on the prescription sheet, and if anything is unclear, ask your doctor. It is also necessary to talk with the patient and find out from him whether he has previously had an allergic reaction to the drug, and how he felt after the injection. Particularly nervous patients should be reassured by explaining in simple words the purpose of administering the drug. Immediately before the injection, you need to wash your hands with soap and treat them with an antiseptic.