D
On October twenty-sixth, 1930,
Vladimir Khavkin
. An outstanding bacteriologist, born in Odessa and worked for many years in British India. His achievements include the creation of vaccines against cholera and plague. Their fates turned out differently. One was considered successful. The attitude towards the other was more restrained. The history of the creation of the anti-cholera vaccine - Khavkin's most labored brainchild - allows us to understand all the difficulties that vaccinologists have faced and may still face from the very beginning of the formation of this science.
Vladimir Aronovich Khavkin was born on March 15, 1860. He early showed an inclination towards biological knowledge and after graduating from high school he entered the natural sciences department of the Faculty of Physics and Mathematics of Novorossiysk University in Odessa. At this time, Ilya Mechnikov
, one of the founders of the development of bacteriology in the Russian Empire.
Vladimir Khavkin became his student and soon demonstrated outstanding success. Bacteriology itself as a science was then taking only its first steps and was in the “romantic” period of hunting for microbes, while the discovery of the supposed causative agents of a particular disease did not at all mean the rapid discovery of ways to combat infection. In the mid-1880s, the name of Louis Pasteur
, who, together with his assistants, managed to create a method of protection against previously incurable rabies.
One of the founders of the development of bacteriology in the Russian Empire Ilya Mechnikov
ok.ru
Taming Rabies
A graduate of the Paris Ecole Normale and a chemist by training, Louis Pasteur became interested in the nature of fermentation and decay and soon established the role of microorganisms in these natural processes. This, as well as the development of practical recommendations for heating nutrient fluids to preserve them (later called pasteurization), determined Pasteur's lifelong interests in the study of microorganisms and the discovery of new ways to combat disease. Pasteur proposed vaccines against anthrax, chicken cholera and swine rubella, and developed recommendations for combating silkworm diseases. By this time, outstanding researchers Emile Roux, Charles Chambernard, Louis Duclos and others were working in Pasteur’s laboratory. Together with them, he took up the problem of rabies. The decision to work specifically on rabies was partly explained by the previous specialization of Pasteur’s laboratory on animal diseases and the successes achieved in this: he chose a disease that is dangerous for people, but which primarily affects animals.
The methods by which Louis Pasteur and his assistants tried to find means of preventing rabies would now probably cause confusion and serious concern among many scientists. While studying anthrax and chicken cholera, Pasteur actually adhered to his own method of developing a vaccine, which involved obtaining a culture of bacilli of reduced and stable virulence. This was achieved by experiments with isolating and isolating bacilli of certain diseases and growing them in certain environments (for example, with reduced or increased access to oxygen) or by exposing the grown crops to some aggressive substance (for example, carbolic acid). As a result, it was determined in what environment it was possible to obtain weakened bacilli from which the vaccine was made.
The methods by which Louis Pasteur and his assistants tried to find means of preventing rabies would now probably cause bewilderment and serious concern among many scientists
However, rabies is caused by a virus, that is, an agent that was technically impossible to identify and isolate at that time. This already directed Pasteur into the field of experiments, which, strictly speaking, contradicted the foundations of the method he had chosen. For a long time, Pasteur and his assistants were methodically infecting various animals with rabies, trying to find a mechanism for weakening the disease (these experiments, as well as the constantly used vivisections, which were widely reported in the press, at one time made Pasteur an anti-hero of the animal rights movement). This was supposed to open the way to the production of a vaccine from nerve tissue preparations (the level of medical knowledge at that time was enough to understand that an invisible pathogen affects the nervous system and brain). Finally, after numerous unsuccessful experiments, laboratory specialists established that the bone marrow preparation of a rabbit that died of rabies loses virulence as it dries in air. And the sequential administration of these drugs of varying degrees of drying protects the animal from further infection with rabies.
It was at this point that Pasteur approached the most dangerous and ethically difficult stage of his research. Until now, all of its vaccines have been intended to prevent veterinary diseases. Now he had to create a remedy that was intended to save people, which means it should be tested on humans. When it became known that Pasteur was experimenting with the treatment of rabies, victims of rabid dog bites who were facing imminent death began to contact the laboratory. For a long time Pasteur could not decide to use an untested remedy with not entirely clear properties. And yet, in 1885, he gave in to the requests of the parents of the Alsatian boy Joseph Meister (Josef Meister), who was severely bitten by a rabid dog. By this time, Pasteur only had confirmed data that dogs who received the rabbit bone marrow vaccine were protected from further infections. However, the scientist apparently had no data on whether a course of such vaccinations helps if the animal has already become infected. Moreover, a number of experimental dogs did not pass the control period of the experiment. Deciding to treat a person with such data in hand, even by the standards of scientific ethics of the 19th century, was a desperate and dubious step. Be that as it may, Pasteur's experiment was a complete success. The maester was healed. It is worth noting that some modern scientists are still not entirely sure whether the dog that bit Meister was really rabid (the conclusion was made only based on the presence of hay and other foreign objects in the dog’s stomach; for an unknown reason, no other tests were taken to confirm the diagnosis). However, all the serious questions about the decisions made in Pasteur’s laboratory do not give reason to deny that he really found a means of protection against rabies. And rabies vaccination using the Pasteur method soon began to be used in France and other countries of the world with obvious success. Pasteur became a national hero of France and soon received at his disposal an institute that was named after him. He had to study the causative agents of diseases and search for means of salvation from them. The Institute attracted ambitious scientists from different countries who, for various reasons, found it difficult to conduct research in their homeland or wanted to be in the leading bacteriological center in the world. Soon Vladimir Khavkin will link his fate with the Pasteur Institute.

Louis Pasteur - French chemist and microbiologist, member of the French Academy
britannica.com
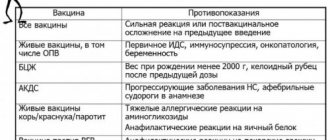
Contraindications for use
Immunoprophylaxis of cholera has certain limitations for the introduction of vaccination.

The following groups of people are not allowed to receive vaccination:
- persons who have acute infectious or inflammatory diseases;
- if gastrointestinal dysfunction is observed. Vaccination is allowed only after the condition has normalized;
- people with tumors of various locations;
- patients who have congenital or acquired immunodeficiency.
The drug is not administered to pregnant women, since its effect on the child and the body of the expectant mother has not been studied.
The Path to Pasteur
Khavkin did not make the decision to leave Russia entirely of his own free will. The public and unspoken rules of the socio-political and academic system in the Russian Empire that existed at that time did not give him the opportunity to freely pursue an academic career. And it wasn’t even a matter of revolutionary hobbies that ruined the lives of many Russian students of those years. Khavkin was indeed close to populist circles, but the movement, apparently, did not capture him. In addition, he was a staunch opponent of the terrorist struggle, to which the southern populists were inclined. Khavkin was also a member of the Jewish self-defense units that tried to organize the protection of civilians from the pogrom that swept through Odessa in the spring of 1881: then there were rumors that after the death of Alexander II, the property of Jews was deprived of the protection of the law. However, despite the temporary arrest (the authorities detained those who took part in the clashes on both sides), this did not create insurmountable obstacles to further scientific work, especially at the freedom-loving and non-capital Novorossiysk University.
The success in identifying Vibrio cholerae and establishing a connection between the disease and the presence of Vibrio in the intestines and discharges of patients belonged to Robert Koch, the great German bacteriologist and long-time rival of Pasteur.
The problem was different: the condition for taking up a teaching position for a talented graduate was baptism. Khavkin, for whom the faith of his fathers remained an important issue, refused to be baptized and went to work at the Odessa Zoological Museum, and then left for Switzerland. Soon, Khavkin’s teacher Ilya Mechnikov believed that he could most effectively continue his bacteriological research at the Pasteur Institute, and in 1887 he moved to Paris, where he immediately received a laboratory. He did not forget about his student and wrote to him in Switzerland, offering to move to the French capital. However, all positions in Mechnikov’s laboratory were already filled out. The Institute had the only unfilled vacancy for a librarian. Khavkin, who idolized Pasteur, was ready for any conditions. In his free time from his duties as a librarian, Khavkin could work in Mechnikov’s laboratory on his research. In fact, this meant working extremely hard in an empty laboratory at night. Khavkin himself recalled how, having discovered some strange effect of his experiments, he was forced to wake up his colleague Alexandre Yersin,
(the future discoverer of the plague bacillus), who meekly agreed to go to the laboratory and record the observed phenomenon.
In 1890, Alexandre Yersin received a position as a ship's doctor in Indochina, and Khavkin was offered his place at the institute - an assistant ( preparateur
) in the laboratory of
Emile Roux
, Pasteur's long-time colleague and one of the creators of the method of treating diphtheria.
A place in the laboratory of a scientist already recognized as great was an offer that Khafkin accepted without hesitation. Roux's position as a laboratory assistant involved a fairly large amount of work: he had to help the scientist prepare materials for his famous training course in bacteriology - Cours de microbie technique
. However, this same preparation meant the need to constantly study leading scientific journals, which helped to become familiar with current discoveries. It was here that Khavkin was able to begin his ambitious research - the development of a vaccine against cholera.

Pasteur Institute in Paris
pasteur.fr
Forward to cholera!
Developing a reliable cure for cholera was truly a monumental task. Although the rabies vaccine brought Pasteur worldwide fame and made him the personification of scientific progress, it is worth recognizing that as a disease, rabies did not pose a serious social problem. It was not transmitted from person to person (more precisely, although this is possible, such cases have not been recorded). It was possible to become infected with rabies only by accident - after meeting a rabid animal. Moreover, a bite from such an animal does not automatically mean infection (much depends on the depth and location of the bite). It is known that at the time the Pasteur vaccine appeared in France, no more than 30 cases of illness and death from rabies were recorded annually. Rather, it was the fear associated both with the severe course of the incurable disease and with the anxious wait, lasting many weeks, whether ominous signs of infection would be revealed after the bite, which created a very special reputation for rabies. And Pasteur's victory over this fear was considered a triumph.
For several years, Khavkin methodically changed the environmental conditions for growing vibrio, either trying to accustom it to an acidic environment, or experimenting with anaerobic conditions, or adjusting the pressure. All these experiments failed
Cholera epidemics, after the disease entered Europe at the beginning of the 19th century, regularly claimed tens and hundreds of thousands of lives. The discovery of a remedy that could reliably prevent such epidemics could bring the vaccine developer real fame as the savior of humanity. At one time, Pasteur himself studied cholera, trying to discover its causative agent, but did not achieve results. The success in identifying Vibrio cholerae and establishing a connection between the disease and the presence of Vibrio in the intestines and discharges of patients belonged to Robert Koch
- the great German bacteriologist and long-time rival of Pasteur. He made his discovery in 1884. After the Franco-Prussian War, the Frenchman Louis Pasteur hated everything connected with Germany and never hid his feelings. His rivalry with Koch became intensely personal, so the creation at the institute of a vaccine against the disease whose causative agent was discovered by Koch would certainly be a spectacular move. Nevertheless, it is hardly surprising that research in such an important area was carried out only by a single laboratory assistant, a Jewish emigrant from Russia. What was known about cholera and Vibrio cholerae, as well as what seemed doubtful and controversial, would make any researcher think twice before embarking on such work.

Cholera vaccination
pikabu.ru
Cholera
Cholera (cholera) is an acute intestinal anthroponotic infection with a fecal-oral transmission mechanism, which is characterized by the development of acute gastroenteritis with water-electrolyte imbalance with the rapid development of dehydration. Refers to particularly dangerous conventional diseases.
History and distribution. Cholera has existed since ancient times. Until the beginning of the 19th century. the disease was recorded within the Hindustan Peninsula and did not spread to other regions. But with the development of trade and transport relations and tourism from the middle of the 19th century, cholera began to spread beyond its historical focus. From 1817 to 1925, six cholera pandemics were recorded. In 1872, the causative agent of cholera Vibriocholerae was discovered by E. Niedzwiecki, but he did not obtain it in pure culture. In 1883, R. Koch described the causative agent of the disease and isolated it in pure culture. From 1926 to 1960, cholera was reported in India and Pakistan and rarely spread to other regions. Since 1961, the beginning of the seventh cholera pandemic has been noted, which is associated with the emergence of a new pathogen Vibrioeltor, which was isolated by F. Gottschlich at the El Tor quarantine station among pilgrims in 1905. Since 1961, WHO began to consider cholera caused by the El Tor vibrio , as a disease that, according to clinical and epidemiological data, does not differ from classical cholera. In the 90s, some researchers predicted the possibility of the beginning of the 8th cholera pandemic, which was associated with the registration of large epidemics and outbreaks caused by Vibrio cholerae serogroup O139 (a synonym for Bengal, indicating its first isolation in the coastal areas of the Bay of Bengal), in the countries of South and South-East Asia. However, WHO experts expressed the view that the threat of the spread of infection is unlikely. After the first publications about Bengal cholera in India, vibrio was isolated in a number of Asian countries: Bangladesh, China, Hong Kong, Malaysia, Burma, Nepal, Singapore and Thailand. 3487 cases of cholera caused by this pathogen were registered; no further large outbreaks were observed. Imports of Bengal cholera without further spread to the USA, Germany, England, Denmark, Estonia, Russia, Japan, Kyrgyzstan, Uzbekistan, Kazakhstan and China were recorded. It is difficult to predict the further development of the spread of the disease, but it is known that epidemic outbreaks of Bengal cholera occur in India and Bangladesh.
Morbidity, mortality. From 1961 to 1992, according to WHO, 2,826,276 cases of cholera were reported worldwide, most of which were caused by Vibrio El Tor. Including 48.1% of cases were noted in Asian countries, 25.7% in America, 26.8% in Africa, 0.2% in Australia, 0.2% of cases in European countries. The mortality rate for cholera in the world (1989–1998) was from 1.8% to 4.7%, with maximum rates in Asia - 5.7%, in Africa - 9.1%, in America - 2.1% and in Europe - 1.7%.
According to the WHO, there are 3–5 million cases of cholera and 100,000–120,000 deaths from cholera each year. Incidence for the period 2004–2008. increased by 24% compared to 2000–2004. In 2008, 190,130 cases of the disease were reported in 56 countries, including 5,143 deaths. However, many cases of the disease remain unreported due to limited surveillance capacity and fears of travel and trade bans. The number of cholera cases annually is estimated at 3–5 million cases and 100,000–120,000 deaths.
The risk of cholera epidemics increases during natural and human-caused disasters, as well as in overcrowded refugee camps. In such conditions, explosive outbreaks of diseases with high mortality rates often occur. For example, in 1994, in refugee camps in Goma, Congo, there were 48,000 cholera cases and 23,800 deaths in one month. Cholera incidence of this magnitude is rare, but it remains a public health problem and causes significant economic and life losses. In 2001, WHO and its Global Outbreak Alert Network partners reported 41 cholera outbreaks in 28 countries.
Cholera outbreaks continue to this day. Classic cholera is recorded in India, Pakistan, Bangladesh, El Tor cholera - in Thailand, Indonesia and other countries of Southeast Asia. Thus, in 2010, 60,240 cases of the disease were detected in Haiti, of which 1,415 were fatal. Pakistan reported in October 2010 99 cases of cholera caused by Vibrio cholerae 01. Currently (2011) in Haiti with 426,785 people turned up with cholera symptoms, 6,169 died, hospital mortality was 1.7%. In the Dominican Republic, the number of cases of cholera is 15.8 thousand people, with 109 deaths. In Ukraine, 33 cases of cholera and 24 cases of vibrio carriage have been registered. Vibrio 01 El-Tor Ogawa was isolated from all patients. Cholera cases were registered in 2011 in Venezuela, Pakistan, Nepal, India, Iran, Nigeria, Somalia, Cameroon, Uganda, the Democratic Republic of the Congo, Afghanistan, and Niger.
In Russia, there has been a stabilization of the epidemic process since 1988, and cholera diseases are mainly imported and sporadic. Over the past 20 years, more than 100 cases of importation have been identified in seven regions of the country. The cholera epidemic in Dagestan in 1994 was severe, when 2,359 people fell ill as a result of the introduction of the disease by pilgrims who performed the Hajj to Saudi Arabia.
Etiology . The causative agent of cholera Vibrio cholerae - belongs to the genus Vibrio, family Vibrionaceae, serogroup 01 of biovars cholerae (classical and eltor). In recent years, up to 80% of all cholera cases have been caused by Vibrio El Tor. Based on their antigenic structure, cholera vibrios are divided into three serovars: Inaba, Ogawa and Gikoshima. Vibrio cholerae has the shape of a comma, due to the presence of a flagellum it has good mobility, is aerobic, does not form spores, is gram-negative, capable of very rapid reproduction, the optimal growth temperature is 37 ° C. It grows well on nutrient media that have a slightly alkaline reaction, liquefies gelatin, decomposes starch, forms indole, reduces nitrates to nitrites, and is lysed by specific phages. Of the pathogenicity factors, the most important is the exotoxin - cholerogens. The pathogen also contains endotoxin, which has a leading role in the development of post-infectious immunity. Vibrio dies when boiled and tolerates low temperatures and freezing. Under the influence of light, air and drying, cholera vibrios die within a few days. Vibrio cholerae is sensitive to chlorine-containing disinfectants. In the water of surface reservoirs, silt and in the body of some hydrobionts, the pathogen not only persists for a long time, but also multiplies. Strains that circulate in the external environment are weakly virulent. On food products, vibrios persist for 2–5 days; on tomatoes and watermelons, when exposed to sunlight, vibrios die after 8 hours. Infection is possible by consuming fish, crayfish, shrimp, oysters caught in polluted waters and not subjected to heat treatment. Vibrios persist for a long time in open reservoirs into which sewage water flows and when the water warms up to more than 17 °C.
In recent years, outbreaks of diarrheal diseases have been recorded that are caused by Vibrio cholerae not of O1, but of O139 serogroup. The course of the disease in its clinical and epidemiological characteristics does not differ from cholera. WHO experts believe that the spread of diseases caused by Vibrio cholerae O139 is becoming a real threat, identical to what happened with Vibrio El Tor in 1961. Vibrios, in relation to cholera phages, are divided into five main phagotypes. There are vibrios that are not agglutinated by polyvalent cholera serum O, the so-called NAG-vibrios, which, by morphological and cultural characteristics, as well as by enzymatic activity, do not differ from cholera vibrios, have the same H-antigen, but belonging to other O-groups . Currently, over 60 serological O-group NAG vibrios have been identified. These vibrios can cause cholera-like diseases.
Epidemiology . The source of infection are patients with a typical or erased form of cholera, vibrio carriers (convalescent, acute, chronic). The pathogen is released into the environment with feces, especially by persons with a typical form of the disease in the first 4–5 days. Patients with erased, atypical forms of the disease are dangerous due to their active lifestyle and contact with others. This is also the epidemic danger of vibrio carriers, but chronic carriage is extremely rare.
The transmission mechanism is fecal-oral, the main route of transmission is water, less often food and household contact. It is important not only to drink water contaminated with the pathogen, but also to use it for washing dishes, vegetables, fruits, and swimming in contaminated water bodies. Cholera has a tendency to spread epidemically. Outbreaks occur more often during the warmer months.
Human susceptibility to cholera is high. People with low acidity of gastric juice, some forms of anemia, helminthic infestations and alcoholism are more often susceptible to the disease. After an illness, type-specific antimicrobial and antitoxic immunity is formed, which persists for one year.
Pathogenesis and pathomorphology. The pathogen enters the human body with contaminated food or water, overcomes the acid barrier, which is facilitated by stomach diseases, which are accompanied by low acidity. Cholera is most severe in people who abuse alcohol or have undergone gastric resection. In the slightly alkaline environment of the small intestine, the vibrio adheres to the border of epithelial cells and multiplies. By adhering to enterocytes, cholera vibrios use the enzyme units of the latter to generate energy for the synthesis of their own structures. It is still controversial whether adhesion itself leads to intestinal secretion. Studies with recombinant, attenuated strains of Vibrio cholerae developed to produce oral vaccines have shown that these strains adhere well but do not cause diarrhea. Vibrio cholerae multiply and produce cholera toxin. There are three toxic substances: 1) endotoxin (lipopolysaccharide); 2) exotoxin (cholerogen); 3) permeability factor. Other toxins of Vibrio cholerae have also been described: zot, which affects the tight junctions of cells and regulates their permeability, as well as the additional toxin ace, which causes an increase in the short circuit current in the Ussing chamber. This is probably the sodium pump blocking toxin reported by Phillips back in the 60s. The location of the genes for these toxins on a chromosome fragment has been revealed. The clinical manifestations of cholera are based on electrolyte diarrhea syndrome. The development of diarrhea consists of hypersecretory processes, which are caused by activation of the enzyme adenylate cyclase in the epithelial cells of the small intestine under the influence of cholerogens and the accumulation of cAMP, leading to increased secretion of water and electrolytes into the intestinal lumen. Studies (D. Powelletal., 1994; CSeurs. G. Kaper., 1996) describe in detail the biochemical properties and biological effects of cholera toxin. Through a system of cyclic nucleotides, it stimulates the secretion of chlorine, inhibits the absorption of electrically neutral sodium chloride by epithelial cells and modulates their cytoskeleton (microtubules), and causes the accumulation of intracellular calcium. This, in turn, determines an increase in the secretory response, since calcium stimulates the formation of cyclic nucleotides. Calcium and the protein calmodulin activate phospholipase, which causes phosphorylation of proteins with an increase in the permeability of the apical membranes of crypt enterocytes, which leads to hypersecretion of water and electrolytes. Bradykinin, kallidin, and vasoactive intestinal peptide influence the increase in the synthesis of cyclic nucleotides. It has been proven that diarrhea also occurs due to the release of serotonin, which in turn stimulates the formation of prostaglandin E2. The role of serotonin as the most important mediator of hypersecretion in the small intestine under the action of cholera toxin is proven by the successful use of serotonin receptor antagonists. In cholera, isotonic dehydration occurs. According to modern concepts, cholera diarrhea is caused by increased secretion of intestinal juice (sodium ions, bicarbonate, potassium chlorine, water), accelerated physiological desquamation of enterocytes, increased membrane permeability, as well as slower reabsorption of sodium, chlorine and water ions. Patients experience: severe metabolic acidosis, blood thickening, increased specific gravity, deterioration of the rheological properties of blood, hypokalemia, increased protein content, etc. Fluid losses with feces and vomit in a short period of time can reach volumes that do not occur with diarrhea of other etiologies . As a consequence of dehydration, significant hemoconcentration, hypovolemia, hypoxia, thrombohemorrhagic syndrome and acute renal failure develop. Additional mechanisms of protection against dehydration and loss of electrolytes are included:
a) a decrease in body temperature - this leads to a decrease in natural perspiration (about 1.5 liters of sweat are lost per day along with sodium, potassium and other electrolytes); b) dryness of the mucous membranes of the mouth, eyes, and genitourinary organs appears (secretion of all glands is reduced); c) oliguria develops up to anuria.
However, these defense mechanisms do not save, since the insidiousness of Vibrio cholerae is that its toxin (cholerogen), when combined with epithelial cell receptors, causes prolonged hypersecretion of fluid and electrolytes from the crypts of the small intestine for 18–24 hours. During this period, the body dies without treatment (rehydration).
The dead often exhibit a “Hippocratic face”: sunken eyes, sharpened facial features, sallow skin color with a bluish tint. The “wrestler or boxer pose” and the “washerwoman’s hand” are often observed. Cadaveric spots are purple-violet in color. The blood has a tar-like consistency that resembles currant jelly. Redistribution of blood and its accumulation in large veins, desolation of the capillary network are revealed. The kidneys decrease in size, the glomeruli are filled with blood, and degeneration of the convoluted and proximal tubules is noted. The intestines are full of fluid. An exudative process is observed throughout the digestive tract, but no signs of inflammation are observed. There are dystrophic changes in the liver and myocardium.
The method of optical and electron microscopy revealed functional changes in the structures of the heart, kidneys, adrenal glands, hypothalamic nuclei and pituitary gland. However, all these changes are secondary, regulatory, protective and are aimed at restoring water-salt homeostasis. These disturbances in cholera are in no way connected with a direct toxic effect on the structures of internal organs, but are caused by dehydration.
It is this approach to understanding the pathogenesis of cholera - recognition of the primacy of dehydration and electrolyte imbalance - that made it possible to develop pathogenetic rehydration therapy, which is aimed at eliminating the main cause of the pathology.
Clinical picture. The incubation period lasts from several hours to 5 days, most often 1–3 days. The disease begins acutely in the middle of full health, often at night with the appearance of rumbling, flatulence and loose stools. The body temperature is often normal, but in some patients it is low-grade. The stool is watery, a cloudy white liquid with floating flakes and resembles “rice water” or “meat slop” in appearance. The act of defecation is painless. Then vomiting of gastric contents follows, soon it becomes watery and also resembles rice water. Cholera is characterized by dehydration, desalination and metabolic acidosis; there are no symptoms of intoxication. In regions with hot climates, where there is a significant loss of fluid and electrolytes through sweat, as well as when water consumption is reduced due to damage to water supplies, cholera is severe due to the development of a mixed mechanism of dehydration, which occurs due to a combination of extracellular (isotonic) dehydration with intracellular (hypertonic) dehydration. In such cases, the frequency of stool does not always correspond to the severity of the disease. Clinical symptoms of dehydration develop with infrequent bowel movements, and in a short time a significant degree of dehydration develops, which threatens the patient’s life.
In 80% of people, cholera occurs in mild or moderate form. 10–20% of people develop severe watery diarrhea with signs of dehydration. In accordance with the classification of cholera by V.I. Pokrovsky, four degrees of dehydration are distinguished: I degree involves fluid loss of up to 3% of body weight, II degree - 4-6%, III degree - 7-9%, IV degree (decompensated dehydration) - 10% or more.
Dehydration of the first degree is detected most often, while many symptoms of the disease are not expressed and the disease is abortive in nature. Some patients experience a prodromal period lasting about a day, which is characterized by dizziness, malaise, weakness, and nausea. The first symptom of the disease is abnormal stool, which is watery in 2/3 of patients and mushy in 1/3. In 5% of patients, the stool may be formed. The frequency of diarrhea is from 5 to 10 times a day. The duration of the disease is no more than 3 days. The bowel movements are not profuse. Vomiting may occur in about half of patients. The skin is moist, turgor is preserved. In 2/3 of patients, dryness of the oral mucosa is detected. There are no hemodynamic disturbances.
Dehydration of the second degree is recorded in approximately 20% of patients. In most cases of the disease, the prodromal period is either not pronounced or short-lived. The disease is characterized by the appearance of loose stools, which quickly become watery and in half of the patients resemble rice water. Vomiting occurs in the first hours of illness, its frequency reaches up to 10 times a day. The total loss of fluid with stage II dehydration averages 5–6 liters. Symptoms of dehydration develop quickly. Characterized by weakness, dizziness, fainting, dry mouth, thirst, hoarseness, decreased skin turgor. A quarter of patients have cyanosis and acrocyanosis. Body temperature is normal or subnormal. An increase in body temperature is rarely detected. The tongue is dry. Half of the patients have tachycardia, a quarter have arterial hypotension, and in some cases oliguria. Some patients experience cramps in the calf muscles, hands and feet. When examining blood, signs of hemoconcentration are minimal (Ht = 0.46–0.50) due to compensatory blood thinning. Electrolyte changes are compensated. Most often, compensated or subcompensated metabolic acidosis (pH 7.36–7.40; BE = -2.0–5.0 mmol/l), hypokalemia, and hypochloremia are observed.
Dehydration of the third degree is detected in 10% of cholera patients during outbreaks. The onset of the disease is acute, and symptoms of dehydration develop quickly - after 10–12 hours. The frequency of stools is up to 20 times a day, bowel movements look like rice water. Vomiting is profuse, more than 20 times a day, the vomit resembles rice water. Patients experience increasing weakness, dry mouth, thirst, agitation, irritability, and muscle cramps in the extremities (most often the calf muscles). A third of patients have subnormal body temperature. The skin is dry, pale. The facial features are pointed, the eyeballs are sunken, and the symptom of “dark glasses” is observed. A decrease in skin turgor is detected in the vast majority of patients.
The voice is changed, hoarse and weakened, speaking in a whisper is typical. Heart sounds are muffled, tachycardia and arterial hypotension are noted. In 3/4 of cases, oliguria occurs, in 1/4 - anuria. Hemoconcentration is moderately pronounced (Ht = 0.50–0.55), decompensated metabolic acidosis (pH 7.30–7.36; BE = -0.5–10.0 mmol/l), hypokalemia, and hypochloremia are noted. In the absence of intensive care, the condition of patients worsens and can lead to death.
Dehydration of the IV degree is the most severe form of cholera, which is called algid. It is more appropriate to call this form of the disease decompensated dehydration, since the body is not able to independently maintain water-salt balance and the activity of functional systems. The disease is characterized by a rapid course, continuous profuse stool and vomiting, with the development of hypovolemic shock, which is one of the manifestations of the disease. Sometimes, with the development of intestinal paresis, diarrhea and vomiting may stop and fluid accumulates in the intestinal lumen. The patients are in a state of prostration, consciousness is preserved. Convulsions, general cyanosis, decreased skin turgor, dry mucous membranes are detected in all patients. Hypothermia, absence of peripheral pulse and blood pressure, tachypnea, anuria and aphonia are noted. The skin is cold and sticky to the touch. Cyanosis becomes purple-black in color. The patient's facial features are pointed, the eyes are sunken, there are bluish circles under the eyes (a symptom of “dark glasses”), the eyeballs are turned upward, and the cheeks are sunken. The nose, cheekbones and chin protrude sharply forward - faсies cholerica. The patient's face and appearance express suffering. Muscle cramps become frequent, periods of relaxation are almost not pronounced. With cramps of the fingers, a spasm in the form of an “obstetrician’s hand” is observed. In some patients, “horse foot” is detected or the foot freezes in a sharply extended position. Spasms of the diaphragm muscles cause painful hiccups.
Patients have hypothermia, body temperature drops to 34.5 °C, the skin loses elasticity - “washerwoman’s hands”. The outcome of the disease is determined by hemodynamic disturbances. The pulse is thready or undetectable, heart sounds are barely audible, heartbeats are arrhythmic. Breathing is rapid, shallow, arrhythmic, 40–60 per minute. In some cases, Kussmaul-type breathing is observed. Anuria is detected in all patients. IV degree dehydration is characterized by hemoconcentration (Ht > 0.55), decompensated metabolic acidosis (pH < 7.30; BE exceeds -10 mmol/l), hypokalemia (up to 2.5 mmol/l). When examining the hemostatic system, increased phases I and II of coagulation, increased fibrinolysis, and thrombocytopenia are revealed. Peripheral blood is characterized by erythrocytosis (up to 7 × 106 in 1 μl), leukocytosis (up to 30–60 × 103 in 1 μl with neutrophilia and a shift of the leukocyte formula to the left). The level of urea and creatinine increases. The ECG reveals signs of pulmonary hypertension with diastolic overload of the right heart and tachycardia.
Sometimes even more rapid development of dehydration is possible. In these cases, dehydration shock develops within several hours (one day), and this form of the disease is called fulminant.
Dry cholera occurs without diarrhea and vomiting, but with signs of rapid development of hypovolemic shock - a sharp drop in blood pressure, the development of tachypnea, shortness of breath, convulsions, aphonia, anuria.
The most severe course of cholera is observed in children under 3 years of age. Children tolerate dehydration worse, and they experience secondary damage to the central nervous system (lethargy, clonic convulsions, convulsions, impaired consciousness up to the development of coma). In children, it is difficult to determine the initial degree of dehydration. It is impossible to rely on the relative density of plasma due to the relatively large extracellular volume of fluid. Therefore, it is advisable to weigh children upon admission to most reliably determine their degree of dehydration. The course of cholera in children has some features: frequent increases in body temperature, more pronounced apathy, adynamia, and a tendency to epileptiform seizures, as hypokalemia quickly develops. The disease lasts from 3 to 10 days, its subsequent manifestations depend on the adequacy of rehydration therapy. When the loss of fluid and electrolytes is replaced, normalization of physiological functions occurs quite quickly and deaths are rare. The main causes of death in case of inadequate treatment of patients are dehydration shock, metabolic acidosis and uremia as a result of acute tubular necrosis.
Along with the severe course of the disease, erased and subclinical forms of the disease are possible, which are revealed during a detailed examination of carriers. Such patients have a history of short-term diarrhea, stool 1-2 times a day. Patients with a subclinical form of the disease are identified in foci of cholera when the pathogen is detected in the feces; they do not have clinical symptoms of the disease, but a blood test reveals an increase in the titer of vibrioid antibodies.
Complications . Among the complications caused by regional circulatory disorders: myocardial infarction, thrombosis of mesenteric vessels, acute cerebrovascular accident. A frequent complication is pneumonia, focal or segmental, in elderly people - hypostatic. Complications include acute renal failure with a predominance of the prerenal form. Exicosis contributes to the development of abscesses, phlegmon and erysipelas. Phlebitis and thrombophlebitis are caused by long-term intravenous rehydration therapy.
Diagnostics . In typical cases of the disease in endemic foci of cholera, the diagnosis does not cause difficulty. Diagnosis becomes difficult when cholera is recorded in an area where it was not previously present and must be confirmed bacteriologically. In areas where cases of cholera have already been registered, patients with cholera and acute intestinal diseases should be actively identified at all stages of medical care, as well as through door-to-door visits by medical workers and sanitary commissioners. If a patient is identified with symptoms of gastrointestinal damage, urgent measures are taken to hospitalize him.
The main method of laboratory diagnosis of cholera is bacteriological examination of stool and vomit in order to isolate the pathogen. If it is impossible to deliver the material to the laboratory in the first 3 hours after collection, then use preservative media (alkaline 1% peptone water, etc.). The material is collected in individual vessels, washed from disinfectant solutions, at the bottom of which a smaller vessel or sheets of parchment paper are placed, disinfected by boiling. The secretions (10–20 ml) are collected using metal spoons into sterile glass jars or test tubes, closed with a tight stopper. In patients with gastroenteritis, material can be taken from the rectum using a rubber catheter. For active collection of material, rectal cotton swabs and tubes are used.
When examining convalescents and healthy individuals who have been in contact with sources of infection, a saline laxative (20–30 g of magnesium sulfate) is first given. All samples for research are delivered in sterile sealed containers with an accompanying person. Each sample is accompanied by a direction in which the first and last name of the patient, the name of the sample, the place and time of collection, the intended diagnosis and the name of the person who took the material are indicated. The indicative test is microscopy of fixed stained smears of stool and vomit. Clusters of vibrios look like schools of fish. Accelerated research methods are immunofluorescence microscopy and the crushed drop method. The research materials are feces, vomit, portions B and C of bile, sectional material, water, food and other environmental objects. To isolate and identify pure culture, enrichment media, selective and differential diagnostic media are used. The results of the express study are obtained after 2–6 hours (approximate answer), accelerated analysis after 8–22 hours (preliminary answer), and full analysis after 36 hours (final answer). Immobilization and microagglutination of vibrios with cholera serum are used as accelerated diagnostic methods; the answer is obtained in a few minutes. All these studies are carried out comprehensively. Serological blood tests (neutralization reaction, enzyme immunoassay) are used in patients with a typical clinical picture of cholera, if Vibrio cholerae is not isolated from feces and vomit. The titers of agglutinins, vibriocidal antibodies and antitoxins are determined. If there are antibody titers (agglutinins 1:40, vibriocidal antibodies 10–4, antienterotoxins - 30 antitoxic units, antimembranotoxins - 50 antitoxic units), cholera should be suspected. The result is positive when the antibody titers in paired sera increase by 4 times. Serological research methods are secondary and are used for retrospective diagnosis.
The presence of Vibrio cholerae in stool is confirmed by laboratory tests. The use of a new rapid diagnostic test (RDT) allows patients to be tested quickly. RDT is currently in the WHO approval process for inclusion in the list of prequalified products. At the same time, in case of positive RDT results, WHO suggests retesting all samples using classical laboratory methods for confirmation. If an outbreak is confirmed, clinical diagnosis based on the WHO standard case definition, with additional testing of selected cases at regular intervals, is sufficient.
Read the end of the article (“Treatment”) in the next issue.
G. K. Alikeeva, Candidate of Medical Sciences N. D. Yushchuk, Doctor of Medical Sciences, Professor, Academician of the Russian Academy of Medical Sciences N. Kh. Safiullina, Candidate of Medical Sciences A. V. Sundukov, Doctor of Medical Sciences, Professor G. M. Kozhevnikova, Doctor medical sciences, professor
MGMSU, Moscow
Contact information for authors for correspondence
The Good Word of the Elder
The causative agent of cholera, despite the terrible consequences of the disease it causes, is extremely vulnerable when exposed to a variety of external factors. It dies instantly in boiling water, dies in direct sunlight, does not tolerate an acidic environment, and is extremely sensitive to various water disinfectants. Actually, if a person drinks water containing vibrios (the main habitat of the bacterium) or eats foods on the surface of which they are found, then the vibrios are likely to die in the hydrochloric acid of the stomach. However, having penetrated the intestines (this is possible if there are a lot of vibrios or if the acidity of a person’s stomach is low) with its alkaline environment, the vibrio begins to multiply rapidly, causing severe consequences for the body: unstoppable diarrhea and a high probability of death from dehydration. Therefore, in order to start working with the causative agent of cholera, it was necessary to provide the vibrio with suitable environmental conditions, and in addition, the vaccine required testing on animals. However, as experience has shown, only humans are susceptible to Vibrio cholerae. Khavkin, who idolized Pasteur, was going to achieve the production of a vaccine using the classic Pasteurian method - obtaining a culture of bacteria of controlled virulence, experimenting with the effects of different environments and then inoculating these cultures into laboratory animals. To carry out such work with an extremely sensitive bacterium, which, as was known, was not capable of infecting any laboratory animal, meant dooming oneself to titanic and, possibly, Sisyphean work.
Khavkin decided to take the most direct and “heroic” path, which was fully consistent with the scientific ethics of the era: he gave himself a subcutaneous injection of a weakened culture of Vibrio cholerae
For several years, Khavkin methodically changed the environmental conditions for growing vibrio, either trying to accustom it to an acidic environment, or experimenting with anaerobic conditions, or adjusting the pressure. All these experiments failed. He tried to grow vibrios in blood serum - which he eventually succeeded in - and then injected this serum into rabbits. Shortly after the injection, the rabbits actually died, but the symptoms of their disease did not resemble cholera at all, and the intestines of the dead rabbits were free of vibrios. Only after carefully studying the dissected corpses of animals that continued to die from the injected serum, Khavkin unexpectedly discovered that the vibrios had settled in the liver and gall bladder, and therefore the nature of the manifestation of the disease was completely different. This led to a series of new experiments on growing Vibrio cholerae in bile. Khavkin tried to inject vibrios from the livers of dead rabbits into other animals, but this did not lead to any effect - the rabbits did not get sick. Khavkin presented the results of the research to Pasteur himself (the Elder, as Khavkin called him in his diary) - he found them interesting, although obscure, and even offered to publish about the experiments, but Khavkin considered that until he received a vibrio culture with stable virulence , it’s better not to think about publication. Pasteur believed that the work could be continued, and thus supported the young researcher. However, for Khavkin, who adored Pasteur and hung on his every word, any attention from a scientific luminary was support. In his memoirs, he, in particular, gave an example of how in the first years of his work at the institute, when Khavkin spent sleepless nights in the laboratory, he was extremely inspired after Pasteur, introducing another delegation to the work of the institute, stopped at the laboratory table Khavkina. The table was littered with piles of notes on endless experiments. Pasteur informed the guests that this worker was doing quite interesting research and, when it was completed, although this was still very far away, there would probably be a “half-page” publication about it.
Pierre Paul Emile Roux - French bacteriologist. Member of the Paris Academy of Sciences, foreign member of the Royal Society of London, foreign honorary member of the Russian Academy of Sciences
Wikipedia
When is the cholera vaccine given?

Due to frequent outbreaks of cholera and a high number of deaths, the incidence rate is monitored by the WHO as well as local health systems. As a preventive measure, vaccination is carried out twice with an interval of 7-10 days for adults, as well as for children aged two years and older.
The injection helps develop immunity in 95% of cases. If there are epidemic indications for vaccination, then re-vaccination is allowed after 3 months. The active ingredients of the cholera vaccine are effective for 6 months. It is recommended to undergo immunization once a year.
Persons traveling to countries that are vulnerable to cholera are also subject to vaccination. Moreover, they must be immunized with cholera monovaccine 6 days before the planned departure date.
All necessary measures aimed at preventing the introduction of dangerous infections from abroad are provided for by special rules for the sanitary protection of borders.
Laboratory assistant and his boss
And yet, this time, Pasteur’s support was limited to only a kind word: Khavkin hoped that the head of the institute would meet him halfway and relieve him of his duties to prepare materials for Emil Roux’s course. But, apparently, Pasteur did not want to open an additional vacancy in the laboratory for this. Roux seemed to be much more skeptical about the prospects of Khafkin’s experiments, which lasted almost two years. Khavkin himself, however, suspected that Ru’s skeptical statements were explained only by the fact that he did not want to lose an assistant on his training course. Khavkin became increasingly burdened by these duties, although he continued to fulfill them conscientiously. In his diary of that time there are entries about how he imagines the scene of a demonstration of a ready-made cholera vaccine in front of the Elder, where he will definitely say that “some gentlemen” did not want to free him from routine work. The painful necessity of working for Ru for a long time determined the attitude of the impressionable and ambitious Khavkin towards the great French explorer. It is worth noting that, although Khavkin suspected Roux of base motives, it was he who ultimately directed his laboratory assistant on a promising path for the development of a vaccine. He informed him about the experiments of the German bacteriologist Richard Pfeiffer
on growing cholera vibrios in the abdominal cavity of guinea pigs and advised repeating this method.
Mechnikov in 1893 decided to drink a glass of water with cholera vibrios. Moreover, with his authority, he convinced several volunteers to join the experiment, assuring them that they were in no danger
Later, Khavkin, taking into account the formed hostility towards Roux, avoided this issue in every possible way and tried to minimize his role in the creation of the vaccine. However, in any case, Khavkin independently did all the necessary enormous work to conduct the experiments. Intraperitoneal injections of vibrio into guinea pigs quickly confirmed their effectiveness. The pigs became infected and died. Although the nature of the disease was not similar to that of humans, nevertheless, as a result of the experiments, it was finally possible to obtain vibrio cultures with controlled virulence - both increased and decreased. They caused the necessary and expected effects in guinea pigs and other laboratory animals. In 1892, Khavkin took the direct road to creating a vaccine. He soon established that subcutaneous injection of first a weakened and then a particularly virulent culture of vibrio into guinea pigs made them immune to vibrios of various strains. This experiment was carried out only on a small number of animals and did not in all cases protect the pigs from death, but Khavkin was in a hurry to report his discovery and already in the summer of 1892 he made a report on the effects obtained. After this, in addition to conducting further experiments with animals, Khavkin decided to immediately begin testing the vaccine on humans.
English bacteriologist Ernst Hankin in India
alchetron.com
Some of the cholera vaccines
The cholera vaccine is included in the World Health Organization's List of Essential Medicines as a vital tool for establishing a basic health system[5]. The cost of immunization against cholera ranges from 0.1 to 4.0 US dollars in different countries[6].
cholera vaccines are currently available (as of 2021):
[7][8][9]:
- Dukoral (Sweden, 1991, synonym WC/rBS) is a monovalent killed whole-cell liquid vaccine. Created on the basis of killed vibrios of serovar O1 serotypes Ogawa (strain 569B) and Inaba classic and El-tor biovars with purified recombinant B-subunit of cholera toxin. Vaccination is two-fold (3-fold for children 2-6 years old), revaccination every 2 years, for children 2-5 years old every 6 months. Short-term effective against toxigenic strains of E. coli. When taking, you need to take it with a buffer solution made from effervescent granules (included). The analogue in China is licensed as OraVacs and is available in capsules, three-time vaccination.
- mORC-Vax (Vietnam, 1997/2009) - a bivalent killed whole cell liquid vaccine, a variant of the Dukoral vaccine licensed in Vietnam, originally produced a modified vaccine that lacked the cholera toxin B subunit and did not require a buffer solution when administered. In 1992, serovar O139 (strain 4260B) was added to the vaccine and the vaccine was renamed ORC-VAX. In 2004, strain 569B was replaced by the Inaba Cairo 48 and Ogawa Cairo 50 strains with a twofold increase in the content of the active substance and the vaccine was registered in Vietnam as mORC-Vax, in India it is produced as Shanchol (since 2009), in Korea it is produced as Euvichol ( since 2015). Vaccination is two-time, revaccination after 2 years, including children from 1 year.
- Vaxchora (USA, 2021) is a live attenuated (weakened microorganism) lyophilized vaccine. Created on the basis of the CVD 103-HgR strain obtained from Inaba strain 569B by removing the ctxA
responsible for the synthesis of subunit A of cholera toxin and introducing the mercury marker
mer
into the
hlyA
responsible for the synthesis of hemolysin. Previously, the vaccine, licensed as Orochol, Orochol E, Mutacol, was produced in different countries, but was discontinued in 2004. Single vaccination for adults (18-64 years old) only; upon administration, it is necessary to suspend it with a buffer solution prepared from powder (included). Requires non-standard cold chain conditions: -15 ÷ -25 °C. - Cholera vaccine inactivated bivalent chemical tablets (Russia, 1992) is a mixture of cholera toxoid with O-antigen obtained from cultures of serovar O1 of the classical biovar strains 569B or KM-76 of the Inaba serotype and M-41 of the Ogawa serotype. Vaccination is a single dose (from 2 years of age), depending on age, 1-3 enteric-coated tablets. Revaccination every 6 months.
Guinea pigs and cholera glass
Khavkin decided to follow the most direct and “heroic” path, which was fully consistent with the scientific ethics of the era. On July 18, 1892, he gave himself a subcutaneous injection of a weakened culture of Vibrio cholerae. According to the observation record, Khavkin recorded only short-term pain at the injection site and a slight rise in temperature, which did not stop him from continuing the experiment. On the twenty-fourth of July, a new injection of a particularly virulent strain followed - it was carried out by Emile Roux. This time the pain was more intense and lasting. The temperature rose to 38.5, but soon all symptoms stopped. Khavkin persuaded three of his acquaintances from Russia to repeat the experiment. Two of them are Georgy Yavein
and
Georgy Tamamshev
- at this time they were interning at the Pasteur Institute, another,
Ivan Vilbushevich
, worked as an engineer. The vaccination was successful. However, of course, there was no need to talk about any end to the tests. French authorities were not going to agree to a wide trial of the vaccine in humans. Khavkin tried to negotiate a trial vaccination in Russia, especially since the Pasteur Institute at that time had good connections with Russia - it was there that the first rabies vaccination station using the Pasteur method was opened outside France. Roux and Pasteur sent a request to the Russian authorities and the Academy of Sciences to assist in selecting 60 people for the experiment and conducting a trial vaccination. However, Russia also did not dare to experiment.
Realizing that the vaccine had not been tested, the English authorities, although they agreed to the experiment in their own colony, still ordered strict adherence to the principle of the voluntary nature of the procedure; English officials also had to ensure that those getting vaccinated were given as clear an explanation as possible of what they would do with them and why
It should be said that not all scientists were convinced by Khavkin’s achievements that a vaccine against cholera had been found. One of the strongest skeptics turned out to be Khavkin’s former teacher Ilya Mechnikov, who believed that vibrio is a necessary but not sufficient condition for the occurrence of cholera and that some still unknown factors that accompany the development of the disease should be investigated. To prove he was right, in 1893 Mechnikov decided to drink a glass of water with vibrio cholera. Moreover, with his authority, he convinced several volunteers to join the experiment, assuring them that they were not in danger. Mechnikov and his secretary, who participated in the experiment, actually escaped with only a slight stomach upset, but the third volunteer contracted severe cholera, which almost led to his death. This forced the scientist to stop the experiment for a while. However, when cholera broke out in Paris in 1894, Mechnikov again began to persuade volunteers to drink a glass of water containing, as it seemed to him, a harmless form of vibrio discovered in a river near Versailles (no cases of cholera were noted there). This time it all ended with the death of one of the volunteers (although the cause of death was not precisely established), which finally forced the Russian scientist to stop his crazy experiments (Mechnikov’s wife later described her husband’s desire to force the volunteers to drink water with cholera vibrios as a special “psychosis ").
Meanwhile, Khavkin, despite the lack of opportunity to conduct large trials, continued to vaccinate some people who wanted it with his experimental vaccine. By and large, at this moment the main “scientific argument” in favor of its effectiveness remained the powerful conviction of the scientist himself that he was on the right path. The further fate of the vaccine was influenced by the fact that among the Khavkin volunteers who were voluntarily vaccinated was a young English bacteriologist, Ernst Hankin,
. Soon he received an appointment to India and believed that the vaccine developed by Khavkin should be tested in India, where cholera was a constant disaster for both the local population and the British living there. It posed a particular danger to British and Indian troops. Hankin began advocating for experimental vaccination in India. To support this idea, he himself went to England and, through a series of lectures, enlisted the support of military doctors. In 1894, the scientist goes to India, where a huge experiment on cholera vaccination begins.

V.A. Khavkin vaccinates children in India
pikabu.ru
Hygiene is more important
Khavkin’s initial assumption was based on the fact that since, according to the general belief, India is a permanent and natural source of cholera, from where the pandemics that have captured Europe begin, vaccinating a certain percentage of the population in this outbreak can reliably solve the world problem.
However, when starting vaccination, Khavkin had no idea how strong immunity the vaccine provides. In addition, it was necessary to convince those wishing to get vaccinated. Realizing that the vaccine had not been tested, the English authorities, although they agreed to the experiment in their own colony, still ordered that the principle of the voluntary procedure be strictly observed; English officials also had to ensure that those being vaccinated were explained, as clearly as possible, what they would do with them and why. Khavkin strictly observed the required conditions, which did not contribute to mass vaccination and did not always allow for accurate observations comparing vaccinated and unvaccinated. In addition, the procedure itself created difficulties: the vaccination had to be carried out twice with a week interval between injections. However, some who received the first dose of the vaccine were afraid of the pain and fever that came with it and simply skipped the next shot. As a result, a quarter of the experiment participants did not receive the full course of the vaccine. Khavkin tried to vaccinate those categories of the population most threatened by cholera: residents of crowded poor neighborhoods and factory workers, but these were representatives of lower castes, subject to rumors and superstitions. The vaccine could not be a complete guarantee against the disease, although it sharply reduced its frequency and spread. The effect of the vaccine expired after a few months, and the method of its manufacture complicated mass vaccination
The sad discovery was that the vaccine provided only temporary immunity, the duration of which did not exceed several months. This still did not make vaccination meaningless, especially during an epidemic, but it still significantly dispelled initial hopes. Finally, one of the problems was the technical capacity to carry out mass vaccination. Khavkin's vaccine was “live” and had to be manufactured locally. In fact, this meant that the scientist himself had to move from place to place with a convoy of guinea pigs. Khavkin heroically accepted all the challenges, but even if he wanted and received powers, he would not be able to travel around the whole of India. For unknown reasons, despite many confirmations received by the time of Khavkin’s work in India that the vaccine could be made from “killed” bacilli (which made transportation much easier), Khavkin continued to adhere to his method. The result of Khavkin's work against cholera should be considered contradictory. He actually created a working vaccine that provided protection against cholera. However, as his own experience showed, the vaccine could not be a complete guarantee against the disease, although it sharply reduced its frequency and spread. The effect of the vaccine expired after a few months, and the method of its manufacture complicated mass vaccination. All this together led British doctors to the conviction that carrying out the minimum necessary sanitary and hygienic measures would be a much better protection against the spread of cholera than the Haffkin vaccine.
Topics: Science and technology