Dexamethasone
Glucocorticosteroid (GCS) is a methylated derivative of fluoroprednisolone, inhibits the release of interleukin-1 and interleukin-2, interferon gamma from lymphocytes and macrophages. It has anti-inflammatory, antiallergic, desensitizing, antishock, antitoxic and immunosuppressive effects.
Suppresses the release of adrenocorticotropic hormone (ACTH) and beta-lipotropin by the pituitary gland, but does not reduce the content of circulating beta-endorphin. Inhibits the secretion of thyroid-stimulating hormone (TSH) and follicle-stimulating hormone (FSH).
Increases the excitability of the central nervous system (CNS), reduces the number of lymphocytes and eosinophils, increases the number of red blood cells (stimulates the production of erythropoietins).
Interacts with specific cytoplasmic receptors, forms a complex that penetrates the cell nucleus, stimulates the synthesis of mRNA, which induces the formation of proteins, incl. lipocortin, which mediate cellular effects. Lipocortin inhibits phospholipase A2, suppresses the release of arachidonic acid and suppresses the synthesis of endoperoxides, Pg, leukotrienes, which contribute to inflammation, allergies, etc.
Protein metabolism:
reduces the amount of protein in plasma (due to globulins) with an increase in the albumin/globulin ratio, increases the synthesis of albumins in the liver and kidneys; enhances protein catabolism in muscle tissue.
Lipid metabolism:
increases the synthesis of higher fatty acids and triglycerides (TG), redistributes fat (accumulation of fat mainly in the shoulder girdle, face, abdomen), leads to the development of hypercholesterolemia.
Carbohydrate metabolism:
increases the absorption of carbohydrates from the gastrointestinal tract (GIT); increases the activity of glucose-6-phosphatase, leading to an increase in the flow of glucose from the liver into the blood; increases the activity of phosphoenolpyruvate carboxylase and the synthesis of aminotransferases, leading to the activation of gluconeogenesis.
Water-electrolyte metabolism:
retains Na+ and water in the body, stimulates the excretion of K+ (MCS activity), reduces the absorption of Ca2+ from the gastrointestinal tract, “washes out” Ca2+ from the bones, increases the excretion of Ca2+ by the kidneys.
The anti-inflammatory effect is associated with inhibition of the release of inflammatory mediators by eosinophils; inducing the formation of lipocortin and reducing the number of mast cells that produce hyaluronic acid; with a decrease in capillary permeability; stabilization of cell membranes and organelle membranes (especially lysosomal ones).
The antiallergic effect develops as a result of suppression of the synthesis and secretion of allergy mediators, inhibition of the release of histamine and other biologically active substances from sensitized mast cells and basophils, a decrease in the number of circulating basophils, suppression of the development of lymphoid and connective tissue, a decrease in the number of T- and B-lymphocytes, mast cells, reducing the sensitivity of effector cells to allergy mediators, inhibiting antibody formation, changing the body's immune response.
In chronic obstructive pulmonary disease (COPD), the action is based mainly on inhibition of inflammatory processes, inhibition of development or prevention of swelling of the mucous membranes, inhibition of eosinophilic infiltration of the submucosal layer of the bronchial epithelium, deposition of circulating immune complexes in the bronchial mucosa, as well as inhibition of erosion and desquamation of the mucous membrane . Increases the sensitivity of beta-adrenergic receptors of small and medium-caliber bronchi to endogenous catecholamines and exogenous sympathomimetics, reduces the viscosity of mucus by inhibiting or reducing its production.
Antishock and antitoxic effects are associated with an increase in blood pressure (due to an increase in the concentration of circulating catecholamines and restoration of the sensitivity of adrenergic receptors to them, as well as vasoconstriction), a decrease in the permeability of the vascular wall, membrane protective properties, and activation of liver enzymes involved in the metabolism of endo- and xenobiotics.
The immunosuppressive effect is due to inhibition of the release of cytokines (interleukin1, interleukin2; interferon gamma) from lymphocytes and macrophages.
Suppresses the synthesis and secretion of ACTH, and secondarily the synthesis of endogenous corticosteroids. Inhibits connective tissue reactions during the inflammatory process and reduces the possibility of scar tissue formation.
The peculiarity of the action is significant inhibition of pituitary function and the almost complete absence of MCS activity. Doses of 1-1.5 mg/day inhibit the adrenal cortex; biological T1/2 - 32-72 hours (duration of inhibition of the hypothalamus-pituitary-adrenal cortex system).
In terms of the strength of glucocorticosteroid activity, 0.5 mg of dexamethasone corresponds to approximately 3.5 mg of prednisone (or prednisolone), 15 mg of hydrocortisone or 17.5 mg of cortisone.
dexamethasone during pregnancy
Girls! This night was simply terrible.. Last night I received hormone tests. I sent them to G, she called back and her first words were: “I almost fell out of my chair, what a nightmare this is!!!”... I have tears in my eyes... I think that’s it...((((arrived.. TTT 2,792 (with lab standards 0.3-4.0) and 17-OPK 2.95 (with norms of 0.93-1.4) Yes, the second one was raised! But he was also upgraded to B! And she didn’t knock him down for me before.. that is , pregnancy occurred on its own, without hormonal pills! And then he tells me to take Eutirox in order to lower TSH, since for B it should be 1.5... And also to lower 17-OPC - dexamethasone... half a tablet a day... Husband I immediately went to the pharmacy and bought it (it was 8 pm).. Moreover, it’s very strange that she prescribed it for me.. She says - drink it if you want, or don’t drink it!!!!! What is this??? Is this the doctor who says this??? As I read the contraindications and instructions for use, I almost lost consciousness!!! So, I started scouring the Internet! Yes, they drink a lot of Dex, but the dose must be strictly selected by an endocrinologist!!! And she is an obstetrician-gynecologist! I was shaking all night... But the last thing I found on the Internet calmed me down a little! This is 17OPK - this is an adrenal hormone, namely, a breakdown product of testosterone. Since it is not directly related to the reproductive system (the adrenal glands are not the reproductive system), then, in general, an endocrinologist should normalize this hormone. But since this hormone is a male hormone and can prevent pregnancy, gynecologists also consider this hormone “theirs.”
This determines the difference in the attitude of gynecologists and endocrinologists to this hormone.
Both agree that an increase in the level of 17OPC is evidence of hyperandrogenism (an imbalance in the level of female and male hormones towards an increase in male hormones in women), however, for such a diagnosis, 17OPC alone is not enough.
Endocrinologists believe that if pregnancy has occurred, then there cannot be hyperandrogenism, because with hyperandrogenism, pregnancy is impossible. Therefore, endocrinologists do not consider it necessary to control, much less reduce, the level of 17OPC during pregnancy, since its increase is a normal process. Moreover, recent studies have shown that the standards available in laboratories are incorrect. Thus, in women under 30 years of age in the first trimester of pregnancy, an increase in 17 OPC to 5.9 ng/ml is allowed, while the forms indicate the norm (which many doctors rely on) to 1.5 ng/ml. Gynecologists have a different point of view: 17OPK, being a male hormone, affects pregnancy. Presumably, an increased level of this hormone leads to cervical insufficiency (sorry prolactin encephalopathy, the medical term has slipped my mind). This is only an assumption, but if there is a threat of miscarriage, this hormone is also checked. Which leads to the prescription of dexamethasone or metipred, while taking large doses of dexamethasone negatively affects the formation of the child’s systems. So, both the child and the mother become prone to diabetes, and the child may develop respiratory failure. This is what I learned from various sources - the Internet, personal conversations with doctors and discussion of this problem on the forum. For the last few years, the country's chief endocrinologist has been persistently trying to convince gynecologists to leave 17 OPC alone, but so far she has had difficulty in doing so.
Today at 7 am I went to a paid clinic, to see the recommended endocrinologist. A very nice woman. I told her everything from the very beginning of planning, how it didn’t work out, what I took... showed her all the hormone tests and what do you think, she said... TSH is basically normal! For B the norm is 2.5 (I have 2.792, and my G said that the norm for B is 1.5) she said you can drink a little Eutyrox, it’s not harmful. But I was shocked about 17-OPK! From the way the doctor prescribed it, and not an endocrinologist, and even if you want to drink it, but don’t drink it if you want... and not even the smallest dose! They drink a quarter, and I immediately drink a half... And at your own peril and risk. And she said such a thing - that an increase in this hormone is evidence of only one disease and until it is lowered it is not for B, accordingly, if B occurs with such a level of the hormone, then this is the norm for your body and you do not have this disease! And there is no need to lower it!
And just look at the tests)) And I retook the TSH test again and 17-OPK. But if it weren’t for B, then it would be necessary to lower it! And this drug is prescribed only when there is a threat..
PS. I just talked to my sister, she also has an elevated 17-OPK level, and she, too, was sick and didn’t take Dex, a wonderful daughter was born!
There was only one conclusion - no scary hormonal drugs without a normal endocrinologist! That's it)
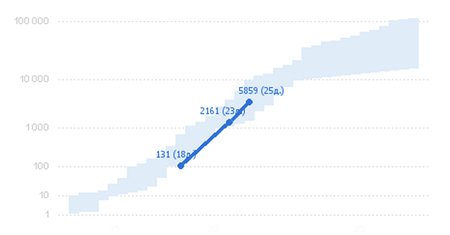
Here is our hCG growth (last today)
Dexamethasone
Dexamethasone is a synthetic hormone of the adrenal cortex, a glucocorticosteroid (GCS), a methylated derivative of fluoroprednisolone. It has anti-inflammatory, antiallergic, desensitizing, antishock, antitoxic and immunosuppressive effects.
Interacts with specific cytoplasmic GCS receptors to form a complex that penetrates the cell nucleus and stimulates the synthesis of matrix ribonucleic acid, the latter induces the formation of proteins, incl. lipocortin, mediating cellular effects. Lipocortin inhibits phospholipase A2, suppresses the release of arachidonic acid and suppresses the synthesis of endoperoxides, prostaglandins, leukotrienes, which contribute to inflammation, allergies, etc.
Protein metabolism:
reduces the amount of protein in plasma (due to globulins) with an increase in the albumin/globulin ratio, increases the synthesis of albumins in the liver and kidneys; enhances protein catabolism in muscle tissue.
Lipid metabolism:
increases the synthesis of higher fatty acids and triglycerides, redistributes fat (fat accumulation occurs mainly in the shoulder girdle, face, abdomen), leads to the development of hypercholesterolemia.
Carbohydrate metabolism:
increases the absorption of carbohydrates from the gastrointestinal tract (GIT); increases the activity of glucose-6-phosphatase, which leads to an increase in the flow of glucose from the liver into the blood; increases the activity of phosphoenolpyruvate carboxylase and the synthesis of aminotransferases, which leads to the activation of gluconeogenesis.
Water-electrolyte metabolism
: retains sodium and water in the body, stimulates the excretion of potassium (mineralocorticoid activity), reduces the absorption of calcium from the gastrointestinal tract, “washes” calcium from the bones, increases the excretion of calcium by the kidneys.
Anti-inflammatory effect
associated with inhibition of the release of inflammatory mediators by eosinophils; inducing the formation of lipocortin and reducing the number of mast cells that produce hyaluronic acid; with a decrease in capillary permeability; stabilization of cell membranes and organelle membranes (especially lysosomal ones).
Antiallergic effect
develops as a result of suppression of the synthesis and secretion of allergy mediators, inhibition of the release of histamine and other biologically active substances from sensitized mast cells and basophils, a decrease in the number of circulating basophils, suppression of the development of lymphoid and connective tissue, a decrease in the number of T- and B-lymphocytes, mast cells, a decrease sensitivity of effector cells to allergy mediators, inhibition of antibody formation, changes in the body's immune response.
In chronic obstructive pulmonary disease, the effect is based mainly on inhibition of inflammatory processes, inhibition of the development or prevention of swelling of the mucous membranes, inhibition of eosinophilic infiltration of the submucosal layer of the bronchial epithelium, deposition of circulating immune complexes in the bronchial mucosa, as well as inhibition of erosion and desquamation of the mucous membrane. Increases the sensitivity of beta-adrenergic receptors of small and medium-caliber bronchi to endogenous catecholamines and exogenous sympathomimetics, reduces the viscosity of bronchial secretions due to inhibition or reduction of its production.
Antishock
and
the antitoxic effect
is associated with an increase in blood pressure (due to an increase in the concentration of circulating catecholamines and restoration of the sensitivity of adrenoreceptors to them, as well as vasoconstriction), a decrease in the permeability of the vascular wall, membrane protective properties, and activation of liver enzymes involved in the metabolism of endo- and xenobiotics.
Immunosuppressive effect
caused by inhibition of the release of cytokines (interleukin-1 and interleukin-2, interferon gamma) from lymphocytes and macrophages. Dexamethasone has a 30 times more pronounced effect than endogenous cortisol. Therefore, it is a more potent inhibitor of the secretion of corticotropin-releasing hormone and adrenocorticotropic hormone (ACTH). In pharmacological doses, it inhibits the hypothalamic-pituitary-adrenal system and promotes the development of secondary adrenal insufficiency. Suppresses the synthesis and release of ACTH by the pituitary gland and, secondarily, the synthesis of endogenous corticosteroids. Inhibits the secretion of thyroid-stimulating hormone and follicle-stimulating hormone. Suppresses the release of beta-lipotropin, but does not reduce the content of circulating beta-endorphin.
Inhibits connective tissue reactions during the inflammatory process and reduces the possibility of scar tissue formation.
Increases the excitability of the central nervous system.
Reduces the number of lymphocytes and eosinophils, increases the number of red blood cells (by stimulating the production of erythropoietins).
The peculiarity of the action is significant inhibition of pituitary function and the almost complete absence of mineralocorticoid activity.