For many women, doctors prescribe Progesterone injections, since this drug is an analogue of the hormone produced by the body.
The medicine is indicated for hormonal disorders during pregnancy, as with its help it is possible to secure and carry the fetus. Doctors should tell patients how Progesterone is injected, as well as how to reduce pain during injections.

Symptoms of hormonal imbalance
A female audience may suspect a hormonal imbalance based on the following characteristic signs:
- mood swings;
- disruption of the menstrual cycle;
- painful sensations in the mammary glands;
- bloating and rumbling in the stomach;
- uterine and vaginal bleeding;
- causeless weight gain, etc.
Important! Having identified such unpleasant symptoms, a woman should consult a doctor and undergo an examination. She definitely needs to donate blood for hormones. If the result determines that the value is exceeded or, conversely, is too low, the specialist will prescribe a course of therapy.
Treatment with progesterone during pregnancy: when and how to do it correctly
In a number of women, repeated spontaneous miscarriages are caused by insufficiency of the progesterone (luteal) phase . Their problem is not a defective egg, but a poor preparation of the uterus to receive a fertilized egg. Usually, insufficiency of the luteal phase is associated with insufficiency of the first phase of the menstrual cycle (estrogen), but if the maturation of the egg has occurred, albeit late, this is already good. Therefore, the second phase becomes more important for implantation.
There are not so many women suffering from luteal phase deficiency; our doctors simply abuse this diagnosis. Firstly, they place it incorrectly. Secondly, the wrong treatment is prescribed.
Often, luteal phase deficiency is diagnosed based on the result of a single test that determines the level of progesterone on the 21st day of the cycle, when the peak production of this hormone should be observed. But the peak occurs not on the 21st day of the cycle, but on the 7th day after the egg matures. Naturally, in women with a menstrual cycle lasting more than 28 days (let me remind you that a duration of up to 35–40 days is considered normal), ovulation will not occur on the 14th day of the cycle, but later. This means that the peak of progesterone levels will also shift and will not be observed on the 21st–22nd day of the cycle.
To make a correct diagnosis, it is necessary to measure progesterone levels at least three to four times during one cycle, and then plot a curve of its levels. This examination should continue for at least three monthly cycles. Moreover, Western doctors make a diagnosis of “luteal phase insufficiency” (especially if a woman has not had spontaneous miscarriages) only after examining the structure of the endometrium, taken on certain days of the second half of the cycle, under a microscope.
Treatment in such cases is prescribed not from the 16th day of the menstrual cycle, but after diagnosed ovulation, which may occur later. Often a combination of sex hormones is used, rather than just progesterone or its synthetic substitute.
Progesterone suppresses the maturation of eggs, so incorrect and untimely administration can aggravate the problem. And you need to take the drug not for five days, but until it is confirmed whether the woman is pregnant or not (before the onset of menstruation). Because if conception occurs, abrupt withdrawal of progesterone on the 25th or other day of the cycle, when the implantation process has already begun, can provoke a miscarriage.
As for artificial insemination , women who have had embryos transferred do not have their own corpus luteum of pregnancy, and therefore there is no organ that will produce progesterone in sufficient quantities until the placenta takes on this role. So it turns out that if after IVF the pregnancy is not supported by additional administration of progesterone, then embryo transfer will in most cases be unsuccessful. You can’t do without this hormone here.
Indications for progesterone injections
When a woman’s body does not generate enough Progesterone, she has problems conceiving. To eliminate this hormonal disorder, patients are prescribed special medications.
Indications for the use of injections of the hormone Progesterone are such pathological conditions as:
- menstrual irregularities;
- pregnancy support in the IVF protocol, preparation of the uterus for the implantation of a fertilized egg;
- periodic bleeding;
- prolonged, heavy and painful periods;
- some diseases of the reproductive system that have an inflammatory etiology and become chronic;
- frequent spontaneous abortions, threat of miscarriage;
- deviations during pregnancy, etc.

Experience with the use of micronized progesterone in the first half of pregnancy
Progesterone is one of the key hormones that ensures the onset and maintenance of pregnancy. Even before fertilization, it causes decidual transformations of the endometrium and prepares it for implantation, promotes the growth and development of the myometrium, its vascularization, and stimulates the growth and development of the mammary glands.
The incidence of abortion, according to various authors, is 10–20%, with 75–80% of them occurring in the first half. Hormonal insufficiency of the ovaries and placenta is one of the most common causes of pregnancy loss. In 64–89% of cases, the main pathogenetic mechanism of miscarriage is progesterone deficiency or a decrease in the receptivity of the uterus and appendages to the action of this hormone. Therefore, treatment of threatened abortion in the first half of pregnancy should be aimed primarily at replenishing the lack of progesterone.
Numerous studies have proven the pathogenetic validity of the administration of progesterone in cases of threatened miscarriage.
Currently, the search continues for optimal drugs based on progesterone and its derivatives, which could be used in obstetrics from early pregnancy and meet high requirements for efficiency, safety and ease of use.
Micronized progesterone - Utrozhestan - is successfully used in the complex treatment of threatened miscarriage in the first half. One of the main advantages of this drug is the possibility of both oral administration and vaginal administration. This dosage form was created to achieve better biological absorption. According to research results, natural micronized progesterone is absorbed quickly and in sufficient quantities. It has been proven that when administered vaginally, the concentration of progesterone in the endometrium increases significantly due to the initial passage of the drug through the uterus.
It should be noted some features of the effect of Utrozhestan on the maternal body and fetus, which constitute its advantage over synthetic analogues. Utrozhestan does not have antigonadotropic activity, androgenic, estrogenic and glucocorticoid properties. It does not affect the lipid profile, blood pressure, carbohydrate metabolism, blood clotting, body weight, and does not cause fluid retention in the body. The main metabolites of Utrozhestan are indistinguishable from the metabolites of endogenous progesterone. When taking the drug, the levels of progesterone metabolites in the blood plasma increase, mainly pregnanediol, pregnanolone, pregnandione, 20α-dihydroprogesterone and 17-hydroxyprogesterone.
As we noted earlier, hormonal disorders are one of the main causes of termination of pregnancy, and the prescription of progesterone as part of complex therapy is undoubtedly pathogenetically justified in these situations. Currently, research is ongoing to optimize the use of progesterone drugs during pregnancy, assess their effectiveness and safety, and their effect on the body of the mother, fetus and newborn.
Purpose of the study
Evaluation of the effectiveness and safety of the use of micronized progesterone (Utrozhestan) by women with threatened miscarriage in the first half of pregnancy.
Materials and research methods
The study included 298 women with clinical signs of threatened miscarriage in the first half of pregnancy. Gestation periods ranged from 7–20 weeks. The average age of women was 27.3 + 5.4 years (25–36 years).
The inclusion criteria for the study were as follows:
- woman's complaints: pain in the lower abdomen and lower back, bleeding from the genital tract;
- external and gynecological examination data: increased uterine tone during palpation, shortening of the cervix during bimanual examination;
- Ultrasound data: increased tone of the uterine walls, the presence of retrochorial and/or retroamnial hematoma, decreased length of the cervix.
All women included in the study were prescribed micronized progesterone (Utrozhestan) vaginally or orally after diagnosis.
Treatment effectiveness criteria were:
- reduction in the severity or disappearance of bleeding and pain, uterine tone (external and vaginal examination);
- lack of uterine tone (ultrasound), reduction in size and/or resorption of retrochorial and retroamnial hematomas.
Side effects and tolerability of the drug were also assessed.
Research results and discussion
Pregnancy was the first in 156 women (52.3%) out of 298 included in the study. In 92 women (30.9%), previous pregnancies ended in spontaneous miscarriages in the early stages or were not developed. 32 (10.7%) had a history of induced abortion. In 18 women (6%), previous pregnancies resulted in live births.
All patients had both subjective and objective symptoms of impending miscarriage. Pain syndrome was observed in 261 women (87.6%), blood discharge from the genital tract was observed in 137 pregnant women (46%), increased myometrial tone (according to ultrasound) was observed in 243 women (81.5%). Hematomas in the uterine cavity were diagnosed by ultrasound in 192 women (64.4%).
All patients received antispasmodic drugs in combination with micronized progesterone (Utrozhestan). The minimum dose of the drug was 200 mg per day, the maximum was 600 mg, depending on the clinical symptoms, taking into account the history and examination of the woman. The average duration of treatment was 87.6 + 9.8 days.
The vaginal or oral route of administration of the drug was determined based on the severity of clinical symptoms, the presence of symptoms of early toxicosis, and the woman’s preference.
The intravaginal route of administration of the drug ensures targeted delivery of progesterone from the vagina to the uterus, which avoids the primary passage through the liver. The active substance is well absorbed and metabolized to a lesser extent, which makes it possible to create a more favorable ratio of the active substance and its metabolites in the blood than when taken orally. As previously conducted randomized studies have shown, in the case of intravaginal use of Utrozhestan, the bioavailability of progesterone is high, individual fluctuations in the level of the hormone in the blood are smaller, and the effective concentration is maintained more stably and for a long time.
Analysis of the effectiveness of treatment showed that the pain syndrome was relieved on average after 3-4 days from the start of taking the drug, blood discharge from the genital tract decreased on average after 2-3 days, and stopped after 5-6 days of treatment.
With dynamic ultrasound, a decrease in myometrial tone was noted in the majority of women (82.7%) on average 6–7 days after the start of therapy. A decrease in the size of retroamnial and retrochorial hematomas was observed 7–10 days after the drug was prescribed in 84.3% of pregnant women.
The effectiveness of micronized progesterone was quite high, since in all women, with the exception of three, pregnancy was maintained until delivery of a viable child. Delivery was timely in 270 women, premature at 32–36 weeks – in 25 (8.5%). All children are alive, growing and developing normally. In two women, the pregnancy did not develop at a period of 7–8 weeks; one pregnant woman had a late spontaneous miscarriage due to the development of chorioamnionitis at a period of 19–20 weeks.
Micronized progesterone was well tolerated. No serious side effects were noted.
With the vaginal route of administration, 13 (4.5%) women initially experienced a slight burning sensation when administering the drug, which went away within 30–40 seconds. Subsequently, these sensations were not repeated.
Taking the drug orally caused mild nausea in 15 women (5%) and dizziness in 25 pregnant women (8.4%). These symptoms ceased after switching to the vaginal route of administration. In general, side effects were not pronounced and were easily manageable.
conclusions
Micronized progesterone (Utrozhestan) is a highly effective means of complex treatment of threatened miscarriage in the first and second trimesters. With its use, the pain syndrome is relieved on average after 3–4 days from the start of taking the drug, blood discharge from the genital tract decreases after an average of 2–3 days, and stops after 5–6 days of treatment.
The duration of therapy and the dose of the administered drug are determined by clinical symptoms, physical examination data, ultrasound results, taking into account the anamnestic data of each individual woman.
The use of micronized progesterone during pregnancy is safe for both the mother and the fetus and can improve the prognosis of pregnancy.
Utrozhestan is highly effective and safe and can be included in complex therapy for the treatment of threatened miscarriage in the first and second trimesters (up to 20 weeks inclusive).
Contraindications
Hormone injections are contraindicated in patients who have pathologies such as:
- any forms of hepatitis;
- malignant neoplasms in the mammary glands;
- liver dysfunction;
- thromboembolism;
- vaginal bleeding, the nature of which cannot be determined;
- lactation period, last month of pregnancy;
- epileptic seizures.
Attention! Progesterone is prescribed with caution to patients who have depression, frequent migraines, diabetes, asthma, serious diseases of the kidneys, liver, heart and blood vessels.
When progesterone is useless
What about a healthy woman ?
If a woman has regular periods and spontaneously becomes pregnant within a year without medical intervention, this is a normal, healthy conception of a child. This means her hormone levels are fine. Why should she be prescribed additional hormonal drugs? It is unlikely that such a woman will have luteal phase deficiency. Read the article Progesterone Nation
If the fertilized egg is full , the pregnancy will progress, so there is no need to administer additional progesterone. If it is defective , the pregnancy will be terminated, and there is nothing wrong with that. Prescribing progesterone will not change the situation.
Scientists from different countries have conducted a lot of research to find out whether it is possible to maintain pregnancy in the early stages, and unanimously claim that there is no “saving” therapy. It does not exist for later stages of pregnancy either. It turns out that all the drugs that have ever been tried to maintain or continue pregnancy are ineffective.
Fortunately, the doses prescribed to pregnant women are so low that they do not have a therapeutic effect, but act as a placebo (dummy). It would seem that what's wrong with this?
The problem is that a woman, often just preparing to become a mother, develops a dependence on all kinds of pills, injections, IVs, etc. And this dependence is supported by artificially created fear - the fear that without drugs the pregnancy will not progress and will end in termination. Thus, taking pills for millions of women becomes an obligatory attribute of life, especially since all their friends, colleagues, and relatives carried their pregnancies “on progesterone.”
The effect of progesterone on the prevention of premature birth in women at risk, as well as with a short cervix, has also been studied for a long time. These women were prescribed progesterone after 24–26 weeks of pregnancy. The first results were encouraging, but recent studies have shown that in this group of women, additional intake of this hormone does not improve the outcome of pregnancy. Today, Western doctors are somewhat confused: should they prescribe progesterone after 24 weeks or not? Most don't prescribe.
Based on all that has been said, we can come to an unambiguous conclusion: with normal conception and normal pregnancy, the female body will independently produce the required amount of progesterone until the placenta completely takes over this function. Additional administration of progesterone just in case is not justified.
Progesterone injections
Women, under no circumstances, should self-prescribe a course of Progesterone therapy. This is the mission of the doctor who will correctly calculate the dosage and duration of treatment.
Typically, their plan includes monitoring the patient’s condition by donating blood for the hormone and Ultrasound examination of the pelvic organs.
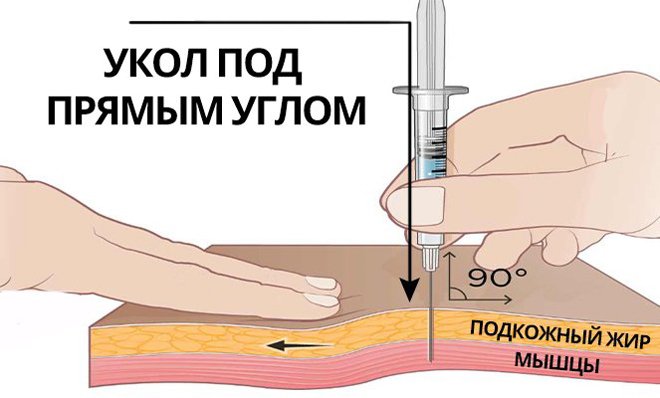
How to give Progesterone injections
The drug is administered intramuscularly, but the instructions indicate that subcutaneous injections can also be given. Before manipulation, you need to warm the ampoule in your palm so that its contents reach a temperature of 40 degrees. After this, you need to wash your hands with soap and wipe them with alcohol.
The drug is drawn into a disposable syringe, the injection site is selected (in the buttocks or abdomen), and wiped with alcohol. The medicine must be administered slowly, despite the pain.
What is the dosage
The dose of the drug is selected by the doctor individually for each patient. In standard cases, the following treatment regimen can be used:
- To start menstruation (if delayed), progesterone is injected in the dosage prescribed by the doctor for seven days.
- To stop vaginal hemorrhages, the drug should be administered within a week, 0.50 ml-1.5 ml.
- For painful periods, 1.00% Progesterone is prescribed in an individually determined dosage for the patient 7 days before the start of the critical days.
Side effects of Progesterone injections
During the course of therapy, patients may experience side effects:
- jaundice develops;
- nausea;
- liver function is disrupted;
- swelling of tissues;
- blood pressure and cholesterol levels increase;
- sexual desire decreases;
- rapidly gaining weight;
- depression develops;
- headache;
- allergic manifestations;
- blood thickens, etc.

Important! If side effects are detected, the woman should consult a doctor who, if there is reason, will discontinue the drug or replace it with an analogue. In severe cases, symptomatic therapy can be carried out.
Effect of Progesterone injections
If the patient does the injections correctly, she will be able to achieve good results in the process of pregnancy planning and infertility treatment:
- the drug helps the embryo to take root;
- reduces the intensity of contractions of muscle tissue in the uterine cavity;
- stops menstruation during pregnancy.
At the same time, the drug begins to rapidly gain weight, and subcutaneous fat actively grows.
If a woman has benign tumors, polyps, cysts, etc., the medicine sometimes provokes their growth. After completion of therapy, patients restoring hormonal levels may be absent from menstrual periods for some time.
Progesterone
Before starting to use the drug Progesterone, it is necessary to conduct a medical examination, including examination of the mammary glands and pelvic organs and a Pap smear examination.
Due to the risk of developing thromboembolic complications, use of the drug should be discontinued if: visual disturbances such as loss of vision, double vision, vascular lesions of the retina occur; migraine; arterial or venous thromboembolism, thrombophlebitis, thrombosis, regardless of location.
If there is a history of thrombophlebitis, the patient should be closely monitored.
The drug Progesterone is used with caution in patients with diseases and conditions that may be aggravated by fluid retention (arterial hypertension, cardiovascular diseases, chronic renal failure, epilepsy, migraine, bronchial asthma); in patients with diabetes mellitus; liver dysfunction of mild to moderate severity; photosensitivity.
Patients with a history of depression should be monitored, and if severe depression develops, the drug should be discontinued.
During long-term treatment with progesterone, regular medical examinations (including liver function tests) are necessary; Treatment should be discontinued if abnormal liver function tests or cholestatic jaundice occur.
When using progesterone, it is possible to reduce glucose tolerance and increase the need for insulin and other hypoglycemic drugs in patients with diabetes mellitus.
If amenorrhea occurs during treatment, pregnancy must be excluded.
In case of acyclic bleeding, the drug should not be used until the cause is determined, including a histological examination of the endometrium.
When using the drug Progesterone with estrogen-containing drugs, you must refer to the instructions for their use regarding the risks of venous thromboembolism.
The use of progesterone may affect the results of some laboratory tests, including liver and thyroid function tests; coagulation parameters; pregnanediol concentration.
Crystals may fall out. If crystals fall out, the ampoule should be heated in a boiling water bath while shaking until the crystals are completely dissolved. If the solution becomes transparent and the crystals do not fall out again when cooled to 36-38 °C, the drug is ready for use.









